

Validation of coding algorithms for the identification of patients with primary biliary cirrhosis using administrative data
- PMID: 20352146
- PMCID: PMC2852223
- DOI: 10.1155/2010/237860
Validation of coding algorithms for the identification of patients with primary biliary cirrhosis using administrative data
Abstract
Background: Large-scale epidemiological studies of primary biliary cirrhosis (PBC) have been hindered by difficulties in case ascertainment.
Objective: To develop coding algorithms for identifying PBC patients using administrative data--a widely available data source.
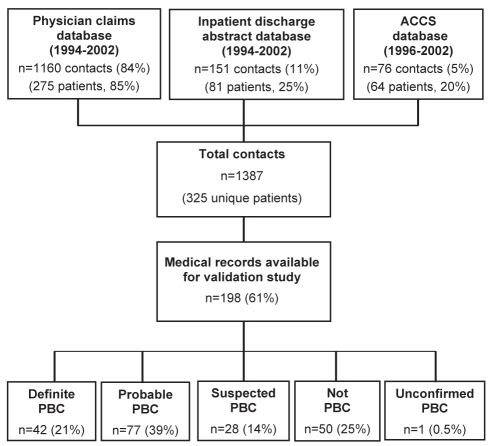
Methods: Population-based administrative databases were used to identify patients with a diagnosis code for PBC from 1994 to 2002. Coding algorithms for confirmed PBC (two or more of antimitochondrial antibody positivity, cholestatic liver biochemistry and/or compatible liver histology) were derived using chart abstraction data as the reference. Patients with a recorded PBC diagnosis but insufficient confirmatory data were classified as 'suspected PBC'.
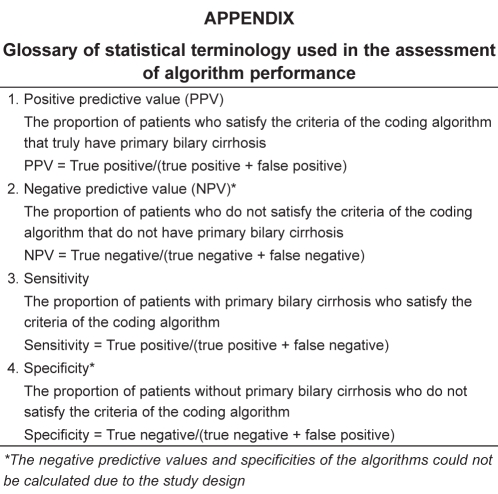
Results: Of 189 potential PBC cases, 119 (60%) had confirmed PBC and 28 (14%) had suspected PBC. The optimal algorithm including two or more uses of a PBC code had a sensitivity of 94% (95% CI 71% to 100%) and positive predictive values of 73% (95% CI 61% to 75%) for confirmed PBC, and 89% (95% CI 82% to 94%) for confirmed or suspected PBC. Sensitivity analyses revealed greater accuracy among women, and with the use of multiple data sources and one or more years of data. Inclusion of diagnosis codes for conditions frequently misclassified as PBC did not improve algorithm performance.
Conclusions: Administrative databases can reliably identify patients with PBC and may facilitate epidemiological investigations of this condition.
HISTORIQUE :: Les études épidémiologiques à grande échelle de la cirrhose biliaire primitive (CBP) sont entravées par des problèmes de détermination des cas.
OBJECTIF :: Élaborer des algorithmes de codage pour repérer les patients atteints de CBP au moyen de données administratives, une source de données largement disponible.
MÉTHODOLOGIE :: Les auteurs ont utilisé des bases de données administratives en population pour dépister des patients ayant obtenu un code diagnostique de CBP entre 1994 et 2002. Ils ont dérivé les algorithmes de codage de CBP confirmée (au moins deux des éléments suivants : positivité aux anticorps antimitochondries, biochimie du foie cholostatique et histologie hépatique compatible) au moyen de données d’abstraction des dossiers en guise de référence. Les patients ayant un diagnostic de CBP établi mais des données de confirmation insuffisantes étaient classés comme « CBP présumée ».
RÉSULTATS :: Sur 189 cas de CBP potentiels, 119 (60 %) avaient une CBP confirmée et 28 (14 %), une CBP présumée. L’algorithme optimal incluant au moins deux usages du code de CBP avait une sensibilité de 94 % (95 % IC 71 % à 100 %) et des valeurs prédictives positives de 73 % (95 % IC 61 % à 75 %) en cas de CBP confirmée, et de 89 % (95 % IC 82 % à 94 %) en cas de CBP confirmée ou présumée. Les analyses de sensibilité ont révélé une plus grande précision chez les femmes et à l’aide de multiples sources de données et d’au moins une année de données. L’inclusion des codes diagnostiques de troubles souvent mal classés comme une CBP n’améliorait pas le rendement de l’algorithme.
CONCLUSIONS :: Les bases de données administratives peuvent permettre de repérer avec fiabilité les patients atteints d’une CBP et faciliter les explorations épidémiologiques de cette maladie.
Figures
Similar articles
-
Identifying Patients With Primary Biliary Cholangitis and Cirrhosis Using Administrative Data in a National Cohort.Pharmacoepidemiol Drug Saf. 2024 Oct;33(10):e70013. doi: 10.1002/pds.70013. Pharmacoepidemiol Drug Saf. 2024. PMID: 39415072
-
Validation of coding algorithms for the identification of patients hospitalized for alcoholic hepatitis using administrative data.BMC Gastroenterol. 2015 Sep 11;15:116. doi: 10.1186/s12876-015-0348-5. BMC Gastroenterol. 2015. PMID: 26362871 Free PMC article.
-
Epidemiology and natural history of primary biliary cirrhosis in a Canadian health region: a population-based study.Hepatology. 2009 Dec;50(6):1884-92. doi: 10.1002/hep.23210. Hepatology. 2009. PMID: 19821525
-
Primary biliary cirrhosis--presentation and diagnosis.Clin Liver Dis. 2003 Nov;7(4):741-58. doi: 10.1016/s1089-3261(03)00101-6. Clin Liver Dis. 2003. PMID: 14594129 Review.
-
Diagnosis and management of primary biliary cirrhosis.Expert Rev Clin Immunol. 2014 Dec;10(12):1667-78. doi: 10.1586/1744666X.2014.979792. Epub 2014 Nov 10. Expert Rev Clin Immunol. 2014. PMID: 25382237 Review.
Cited by
-
Race/Ethnicity and Insurance-Specific Disparities in In-Hospital Mortality Among Adults with Primary Biliary Cholangitis: Analysis of 2007-2014 National Inpatient Sample.Dig Dis Sci. 2020 Feb;65(2):406-415. doi: 10.1007/s10620-019-05809-x. Epub 2019 Sep 5. Dig Dis Sci. 2020. PMID: 31489564
-
Epidemiology and liver transplantation burden of primary biliary cholangitis: a retrospective cohort study.CMAJ Open. 2018 Dec 21;6(4):E664-E670. doi: 10.9778/cmajo.20180029. Print 2018 Oct-Dec. CMAJ Open. 2018. PMID: 30578275 Free PMC article.
-
Developing model-based algorithms to identify screening colonoscopies using administrative health databases.BMC Med Inform Decis Mak. 2013 Apr 10;13:45. doi: 10.1186/1472-6947-13-45. BMC Med Inform Decis Mak. 2013. PMID: 23574795 Free PMC article.
-
A nationwide study of primary biliary cholangitis prevalence, geographic distribution, and health care providers.Hepatol Commun. 2025 Apr 14;9(5):e0677. doi: 10.1097/HC9.0000000000000677. eCollection 2025 May 1. Hepatol Commun. 2025. PMID: 40227093 Free PMC article.
-
Hepatic real-world outcomes with obeticholic acid in primary biliary cholangitis (HEROES): A trial emulation study design.Hepatology. 2025 Jun 1;81(6):1647-1659. doi: 10.1097/HEP.0000000000001174. Epub 2025 Jan 3. Hepatology. 2025. PMID: 39630028 Free PMC article. Clinical Trial.
References
-
- Lindor KD, Gershwin ME, Poupon R, Kaplan M, Bergasa NV, Heathcote EJ. Primary biliary cirrhosis. Hepatology. 2009;50:291–308. - PubMed
-
- Leung PS, Chuang DT, Wynn RM, et al. Autoantibodies to BCOADC-E2 in patients with primary biliary cirrhosis recognize a conformational epitope. Hepatology. 1995;22:505–13. - PubMed
-
- Gross RG, Odin JA. Recent advances in the epidemiology of primary biliary cirrhosis. Clin Liver Dis. 2008;12:289–303. - PubMed
-
- Metcalf J, James O. The geoepidemiology of primary biliary cirrhosis. Semin Liver Dis. 1997;17:13–22. - PubMed
-
- Witt-Sullivan H, Heathcote J, Cauch K, et al. The demography of primary biliary cirrhosis in Ontario, Canada. Hepatology. 1990;12:98–105. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources