

WHO guidelines for antimicrobial treatment in children admitted to hospital in an area of intense Plasmodium falciparum transmission: prospective study
- PMID: 20354024
- PMCID: PMC2847687
- DOI: 10.1136/bmj.c1350
WHO guidelines for antimicrobial treatment in children admitted to hospital in an area of intense Plasmodium falciparum transmission: prospective study
Abstract
Objectives: To assess the performance of WHO's "Guidelines for care at the first-referral level in developing countries" in an area of intense malaria transmission and identify bacterial infections in children with and without malaria.
Design: Prospective study.
Setting: District hospital in Muheza, northeast Tanzania.
Participants: Children aged 2 months to 13 years admitted to hospital for febrile illness.
Main outcome measures: Sensitivity and specificity of WHO guidelines in diagnosing invasive bacterial disease; susceptibility of isolated organisms to recommended antimicrobials.
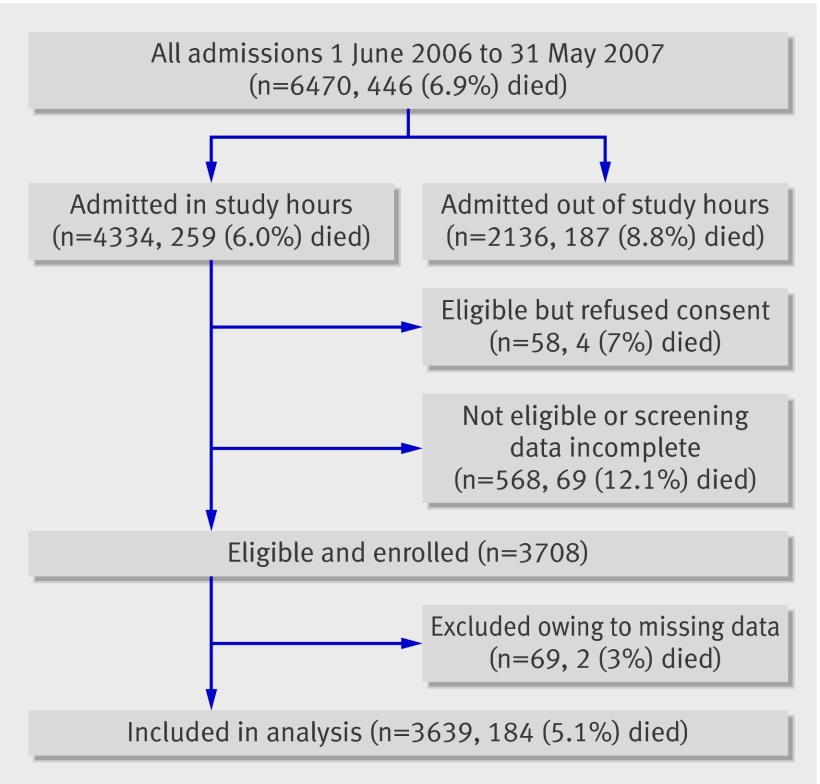
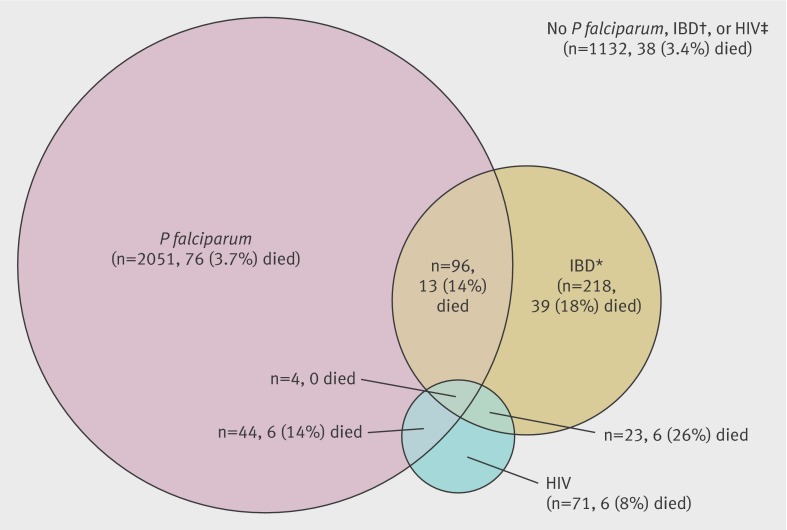
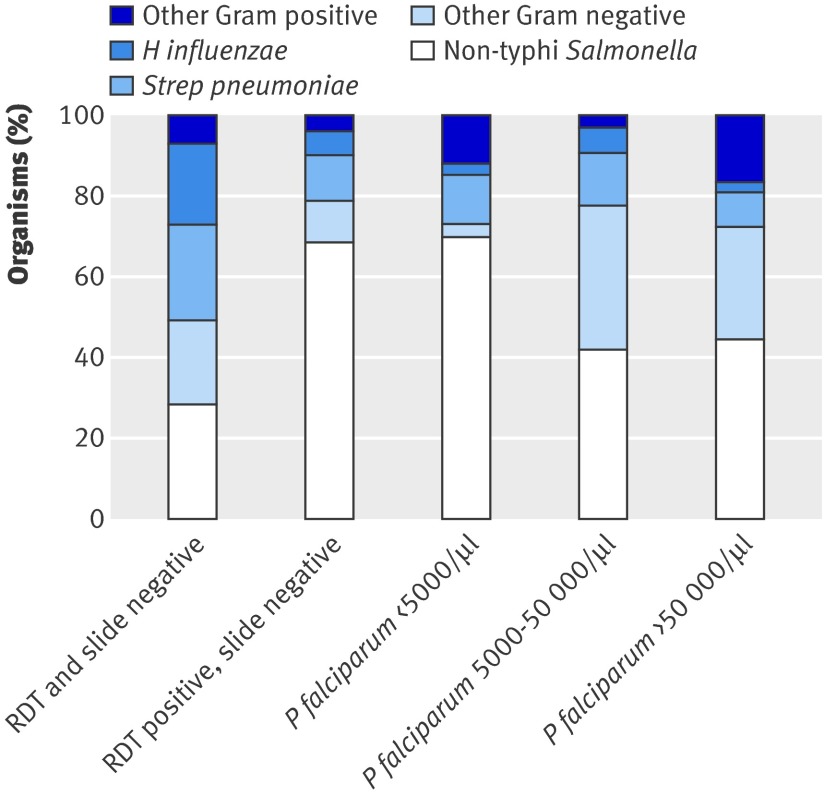
Results: Over one year, 3639 children were enrolled and 184 (5.1%) died; 2195 (60.3%) were blood slide positive for Plasmodium falciparum, 341 (9.4%) had invasive bacterial disease, and 142 (3.9%) were seropositive for HIV. The prevalence of invasive bacterial disease was lower in slide positive children (100/2195, 4.6%) than in slide negative children (241/1444, 16.7%). Non-typhi Salmonella was the most frequently isolated organism (52/100 (52%) of organisms in slide positive children and 108/241 (45%) in slide negative children). Mortality among children with invasive bacterial disease was significantly higher (58/341, 17%) than in children without invasive bacterial disease (126/3298, 3.8%) (P<0.001), and this was true regardless of the presence of P falciparum parasitaemia. The sensitivity and specificity of WHO criteria in identifying invasive bacterial disease in slide positive children were 60.0% (95% confidence interval 58.0% to 62.1%) and 53.5% (51.4% to 55.6%), compared with 70.5% (68.2% to 72.9%) and 48.1% (45.6% to 50.7%) in slide negative children. In children with WHO criteria for invasive bacterial disease, only 99/211(47%) of isolated organisms were susceptible to the first recommended antimicrobial agent.
Conclusions: In an area exposed to high transmission of malaria, current WHO guidelines failed to identify almost a third of children with invasive bacterial disease, and more than half of the organisms isolated were not susceptible to currently recommended antimicrobials. Improved diagnosis and treatment of invasive bacterial disease are needed to reduce childhood mortality.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Antimicrobials in children admitted to hospital in malaria endemic areas.BMJ. 2010 Apr 8;340:c1818. doi: 10.1136/bmj.c1818. BMJ. 2010. PMID: 20378631 No abstract available.
References
-
- Bryce J, Boschi-Pinto C, Shibuya K, Black RE. WHO estimates of the causes of death in children. Lancet 2005;365:1147-52. - PubMed
-
- Berkley JA, Mwangi I, Mellington F, Mwarumba S, Marsh K. Cerebral malaria versus bacterial meningitis in children with impaired consciousness. QJM 1999;92:151-7. - PubMed
-
- Brent AJ, Oundo JO, Mwangi I, Ochola L, Lowe B, Berkley JA. Salmonella bacteremia in Kenyan children. Pediatr Infect Dis J 2006;25:230-6. - PubMed
-
- English M, Punt J, Mwangi I, McHugh K, Marsh K. Clinical overlap between malaria and severe pneumonia in African children in hospital. Trans R Soc Trop Med Hyg 1996;90:658-62. - PubMed
-
- Evans JA, Adusei A, Timmann C, May J, Mack D, Agbenyega T, et al. High mortality of infant bacteraemia clinically indistinguishable from severe malaria. QJM 2004;97:591-7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical