

Megestrol acetate versus metronomic cyclophosphamide in patients having exhausted all effective therapies under standard care
- PMID: 20354522
- PMCID: PMC2856003
- DOI: 10.1038/sj.bjc.6605623
Megestrol acetate versus metronomic cyclophosphamide in patients having exhausted all effective therapies under standard care
Abstract
Background: To evaluate the antitumour activity and safety of metronomic cyclophosphamide vs megestrol acetate in progressive and advanced cancer patients having exhausted all effective therapies under standard care.
Methods: Patients were randomly assigned to receive orally metronomic cyclophosphamide (50 mg b.i.d) or megestrol acetate (160 mg only daily) until intolerance or progression (RECIST 1.0). The primary efficacy end point was a 2-month progression-free rate (PFR(2m)). According to Optimal Simon's design and the following assumptions, namely, P0=5%, P1=20%, alpha=beta=10%, the treatment is considered as effective if atleast 5 out of 44 patients achieved PFR(2m).
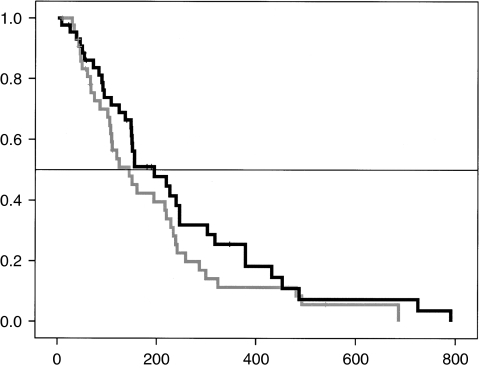
Results: Between September 2006 and January 2009, 88 patients were enrolled. Two patients experienced grade 3-4 toxicities in each arm (4%). One toxic death occurred in the megestrol acetate arm as a consequence of thrombosis. The metronomic cyclophosphamide arm reached the predefined level of efficacy with a PFR(2m) rate of 9 out of 44 and a PFR(4m) rate of 5 out of 44. The MA arm failed to achieve the level of efficacy with a PFR(2m) of 4 out of 44 and a PFR(4m) of 1 out of 44. The median overall survival was 195 and 144 days in the metronomic cyclophosphamide arm and megestrol acetate arm, respectively.
Conclusion: Metronomic cyclophosphamide is well tolerated and provides stable disease in such vulnerable and poor-prognosis cancer patients. This regimen warrants further evaluations.
Figures
References
-
- Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, Filiberti A, Flechtner H, Fleishman SB, De Haes JCJM, Kaasa S, Klee M, Osoba D, Razavi D, Rofe PB, Schraub S, Sneeuw K, Sullivan M, Takeda F (1993) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85: 365–376 - PubMed
-
- Arkenau HT, Barriuso J, Olmos D, Ang JE, De Bono I, Judson I, Kaye S (2009) Prospective validation of a prognostic score to improve patient selection for oncology phase I trials. J Clin Oncol 27: 2692–2696 - PubMed
-
- Berenstein EG, Ortiz Z (2005) Megestrol acetate for the treatment of anorexia-cachexia syndrome. Cochrane Database Syst Rev 13(2): CD004316 - PubMed
-
- Browder T, Butterfield CE, Kraling BM, Shi B, Marshall B, O’Reilly MS, Folkman J (2000) Anti-angiogenic scheduling of chemotherapy improves efficacy against experimental drug-resistant cancer. Cancer Res 60: 1878–1886 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
