

Severe obesity, gestational weight gain, and adverse birth outcomes
- PMID: 20357043
- PMCID: PMC2869513
- DOI: 10.3945/ajcn.2009.29008
Severe obesity, gestational weight gain, and adverse birth outcomes
Abstract
Background: The 2009 Institute of Medicine (IOM) Committee to Reevaluate Gestational Weight Gain Guidelines concluded that there were too few data to inform weight-gain guidelines by obesity severity. Therefore, the committee recommended a single range, 5-9 kg at term, for all obese women.
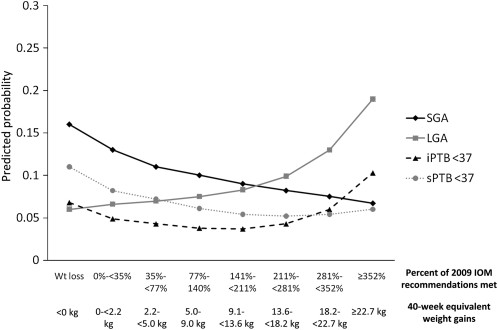
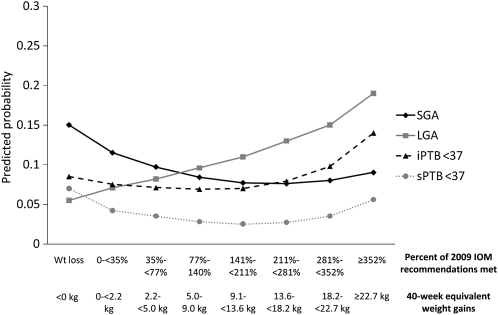
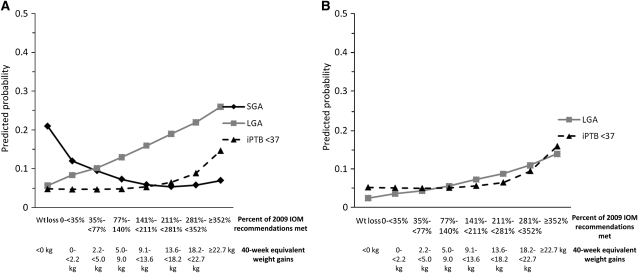
Objective: We explored associations between gestational weight gain and small-for-gestational-age (SGA) births, large-for-gestational-age (LGA) births, spontaneous preterm births (sPTBs), and medically indicated preterm births (iPTBs) among obese women who were stratified by severity of obesity.
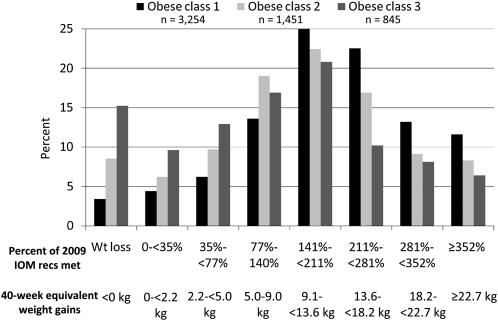
Design: We studied a cohort of singleton, live-born infants without congenital anomalies born to obesity class 1 (prepregnancy body mass index [BMI (in kg/m(2))]: 30-34.9; n = 3254), class 2 (BMI: 35-39.9; n = 1451), and class 3 (BMI: > or =40; n = 845) mothers. We defined the adequacy of gestational weight gain as the ratio of observed weight gain to IOM-recommended gestational weight gain.
Results: The prevalence of excessive gestational weight gain declined, and weight loss increased, as obesity became more severe. Generally, weight loss was associated with an elevated risk of SGA, iPTB, and sPTB, and a high weight gain tended to increase the risk of LGA and iPTB. Weight gains associated with probabilities of SGA and LGA of < or =10% and a minimal risk of iPTB and sPTB were as follows: 9.1-13.5 kg (obesity class 1), 5.0-9 kg (obesity class 2), 2.2 to <5.0 kg (obesity class 3 white women), and <2.2 kg (obesity class 3 black women).
Conclusion: These data suggest that the range of gestational weight gain to balance risks of SGA, LGA, sPTB, and iPTB may vary by severity of obesity.
Figures
References
-
- Freedman DS, Khan LK, Serdula MK, Galuska DA, Dietz WH. Trends and correlates of class 3 obesity in the United States from 1990 through 2000. JAMA 2002;288:1758–61 - PubMed
-
- Sturm R.Increases in clinically severe obesity in the united states, 1986-2000. Arch Intern Med 2003;163:2146–8 - PubMed
-
- Weight Gain During Pregnancy IOM Reexamining the guidelines. Washington, DC: National Academies Press, 2009 - PubMed
-
- Salihu HM, Alio AP, Wilson RE, Sharma PP, Kirby RS, Alexander GR. Obesity and extreme obesity: new insights into the black-white disparity in neonatal mortality. Obstet Gynecol 2008;111:1410–6 - PubMed
-
- Thompson D, Graham C, Burch D, Watson A, Phelps A. Pregnancy related mortality associated with obesity in Florida 1999 through 2002. Tallahassee, FL: Florida Department of Health, Division of Family Health Services, Bureau of Family and Community Health, 2005
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
