

Race and colorectal cancer disparities: health-care utilization vs different cancer susceptibilities
- PMID: 20357245
- PMCID: PMC2857802
- DOI: 10.1093/jnci/djq068
Race and colorectal cancer disparities: health-care utilization vs different cancer susceptibilities
Abstract
Background: It is unclear whether the disproportionately higher incidence and mortality from colorectal cancer among blacks compared with whites reflect differences in health-care utilization or colorectal cancer susceptibility.
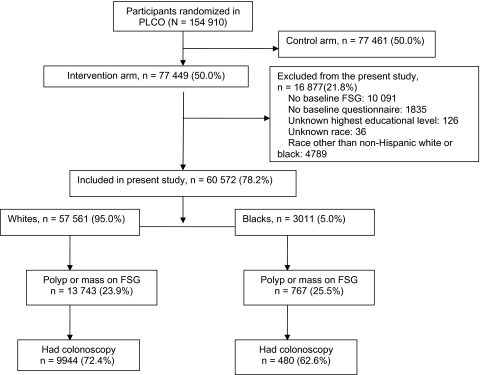
Methods: A total of 60, 572 non-Hispanic white and black participants in the ongoing Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial underwent trial-sponsored screening flexible sigmoidoscopy (FSG) without biopsy at baseline in 10 geographically dispersed centers from November 1993 to July 2001. Subjects with polyps or mass lesions detected by FSG were referred to their physicians for diagnostic workup, the cost of which was not covered by PLCO. The records of follow-up evaluations were collected and reviewed. We used log binomial modeling with adjustment for age, education, sex, body mass index, smoking, family history of colorectal cancer, colon examination within previous 3 years, personal history of polyps, and screening center to examine whether utilization of diagnostic colonoscopy and yield of neoplasia differed by race.
Results: Among 57 561 whites and 3011 blacks who underwent FSG, 13,743 (23.9%) and 767 (25.5%) had abnormal examinations, respectively. A total of 9944 (72.4%) whites and 480 (62.6%) blacks had diagnostic colonoscopy within 1 year following the abnormal FSG screening. When compared with whites, blacks were less likely to undergo diagnostic evaluation (adjusted risk ratio = 0.88, 95% confidence interval = 0.83 to 0.93). Overall, among subjects with diagnostic colonoscopy (n = 10 424), there was no statistically significant difference by race in the prevalence of adenoma, advanced adenoma, advanced pathology in small adenomas (high-grade dysplasia or villous histology in adenomas <10 mm), or colorectal cancer.
Conclusions: We observed a lower follow-up for screen-detected abnormalities among blacks when compared with whites but little difference in the yield of colorectal neoplasia. Health-care utilization may be playing more of a role in colorectal cancer racial disparity than biology.
Figures
Comment in
-
Racial disparities in outcomes of colorectal cancer screening: biology or barriers to optimal care?J Natl Cancer Inst. 2010 Apr 21;102(8):511-3. doi: 10.1093/jnci/djq089. Epub 2010 Mar 31. J Natl Cancer Inst. 2010. PMID: 20357246 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58(2):71–96. - PubMed
-
- Ries LAG, Melbert D, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2005. Bethesda, MD: National Cancer Institute; 2008. Based on November 2007 SEER data submission, posted to the SEER Web site. http://seer.cancer.gov/csr/1975_2005/. Accessed March 24, 2009.
-
- Siegel RL, Jemal A, Thun MJ, Hao Y, Ward EM. Trends in the incidence of colorectal cancer in relation to county-level poverty among blacks and whites. J Natl Med Assoc. 2008;100(12):1441–1444. - PubMed
-
- Doubeni CA, Field TS, Buist DS, et al. Racial differences in tumor stage and survival for colorectal cancer in an insured population. Cancer. 2007;109(3):612–620. - PubMed
Publication types
MeSH terms
Grants and funding
- N01-CN-25524/CN/NCI NIH HHS/United States
- N01-CN-25513/CN/NCI NIH HHS/United States
- N01-CN-25511/CN/NCI NIH HHS/United States
- N01-CN-75022/CN/NCI NIH HHS/United States
- N01-CN-25514/CN/NCI NIH HHS/United States
- N01-CN-25512/CN/NCI NIH HHS/United States
- N01-CN-25515/CN/NCI NIH HHS/United States
- K01 CA127118/CA/NCI NIH HHS/United States
- N01-CN-25476/CN/NCI NIH HHS/United States
- N01-CN-25518/CN/NCI NIH HHS/United States
- N01-CN-25516/CN/NCI NIH HHS/United States
- R01 CA151736/CA/NCI NIH HHS/United States
- N01-CN-25404/CN/NCI NIH HHS/United States
- U01 CA151736/CA/NCI NIH HHS/United States
- N01-CN-25522/CN/NCI NIH HHS/United States
