

Prospective monitoring of cefepime in intensive care unit adult patients
- PMID: 20359352
- PMCID: PMC2887166
- DOI: 10.1186/cc8941
Prospective monitoring of cefepime in intensive care unit adult patients
Abstract
Introduction: Cefepime has been associated with a greater risk of mortality than other beta-lactams in patients treated for severe sepsis. Hypotheses for this failure include possible hidden side-effects (for example, neurological) or inappropriate pharmacokinetic/pharmacodynamic (PK/PD) parameters for bacteria with cefepime minimal inhibitory concentrations (MIC) at the highest limits of susceptibility (8 mg/l) or intermediate-resistance (16 mg/l) for pathogens such as Enterobacteriaceae, Pseudomonas aeruginosa and Staphylococcus aureus. We examined these issues in a prospective non-interventional study of 21 consecutive intensive care unit (ICU) adult patients treated with cefepime for nosocomial pneumonia.
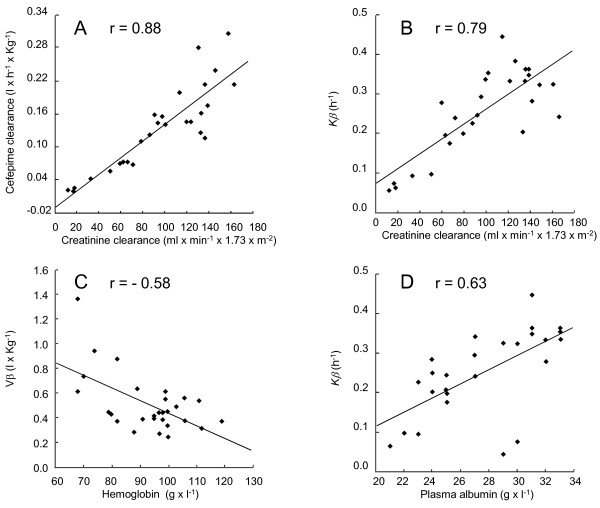
Methods: Patients (median age 55.1 years, range 21.8 to 81.2) received intravenous cefepime at 2 g every 12 hours for creatinine clearance (CLCr) >or= 50 ml/min, and 2 g every 24 hours or 36 hours for CLCr < 50 ml/minute. Cefepime plasma concentrations were determined at several time-points before and after drug administration by high-pressure liquid chromatography. PK/PD parameters were computed by standard non-compartmental analysis.
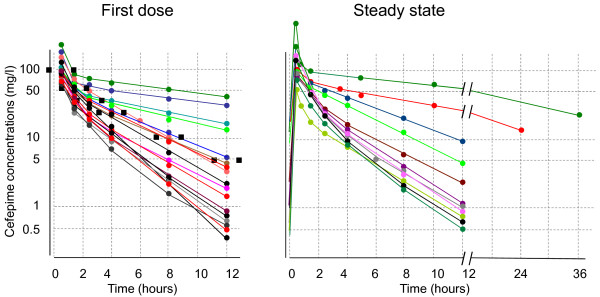
Results: Seventeen first-doses and 11 steady states (that is, four to six days after the first dose) were measured. Plasma levels varied greatly between individuals, from two- to three-fold at peak-concentrations to up to 40-fold at trough-concentrations. Nineteen out of 21 (90%) patients had PK/PD parameters comparable to literature values. Twenty-one of 21 (100%) patients had appropriate duration of cefepime concentrations above the MIC (T>MIC >or= 50%) for the pathogens recovered in this study (MIC <or= 4 mg/l), but only 45 to 65% of them had appropriate coverage for potential pathogens with cefepime MIC >or= 8 mg/l. Moreover, 2/21 (10%) patients with renal impairment (CLCr < 30 ml/minute) demonstrated accumulation of cefepime in the plasma (trough concentrations of 20 to 30 mg/l) in spite of dosage adjustment. Both had symptoms compatible with non-convulsive epilepsy (confusion and muscle jerks) that were not attributed to cefepime-toxicity until plasma levels were disclosed to the caretakers and symptoms resolved promptly after drug arrest.
Conclusions: These empirical results confirm the suspected risks of hidden side-effects and inappropriate PK/PD parameters (for pathogens with upper-limit MICs) in a population of ICU adult patients. Moreover, it identifies a safety and efficacy window for cefepime doses of 2 g every 12 hours in patients with a CLCr >or= 50 ml/minute infected by pathogens with cefepime MICs <or= 4 mg/l. On the other hand, prompt monitoring of cefepime plasma levels should be considered in case of lower CLCr or greater MICs.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
