

Value of symptoms and additional diagnostic tests for colorectal cancer in primary care: systematic review and meta-analysis
- PMID: 20360221
- PMCID: PMC2848719
- DOI: 10.1136/bmj.c1269
Value of symptoms and additional diagnostic tests for colorectal cancer in primary care: systematic review and meta-analysis
Abstract
Objective: To summarise available evidence on diagnostic tests that might help primary care physicians to identify patients with an increased risk for colorectal cancer among those consulting for non-acute lower abdominal symptoms.
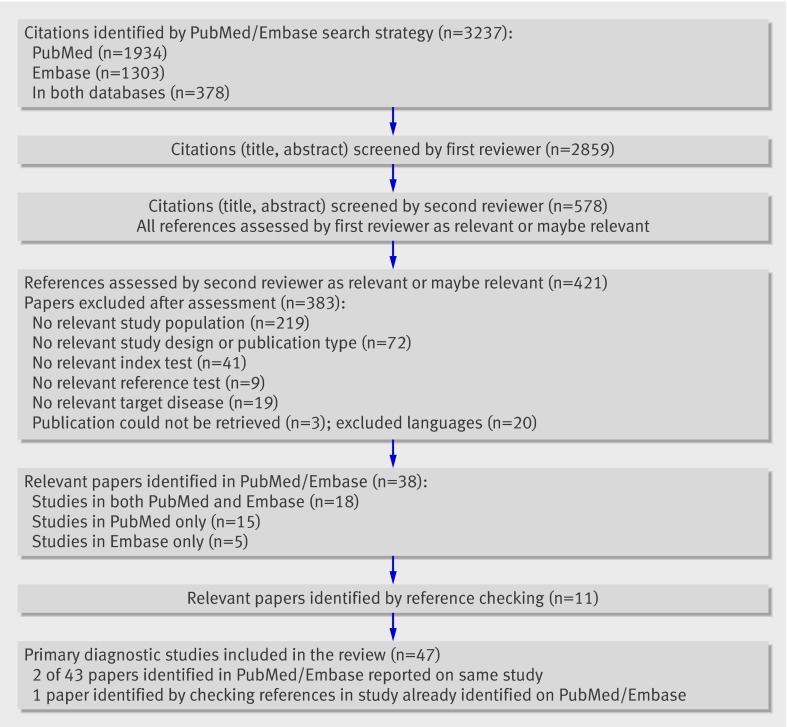
Data sources: PubMed, Embase, and reference screening. Study eligibility criteria Studies were selected if the design was a diagnostic study; the patients were adults consulting because of non-acute lower abdominal symptoms; tests included signs, symptoms, blood tests, or faecal tests. Study appraisal and synthesis methods Two reviewers independently assessed quality with a modified version of the QUADAS tool and extracted data. We present diagnostic two by two tables and pooled estimates of sensitivity and specificity. We refrained from pooling when there was considerable clinical or statistical heterogeneity.
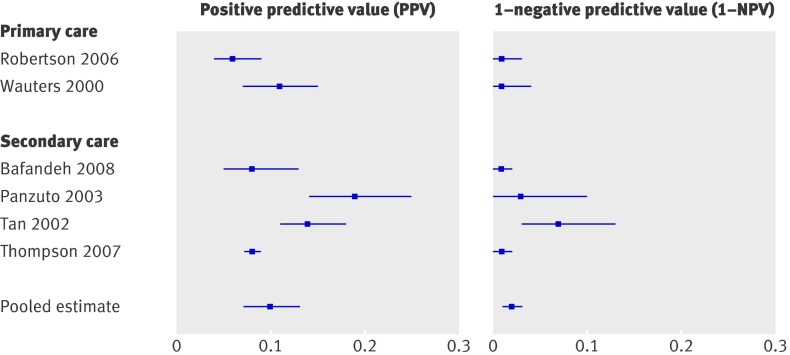
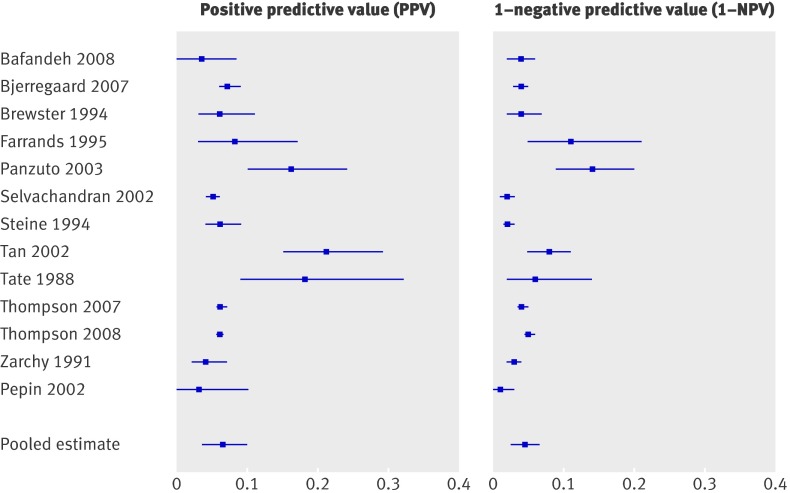
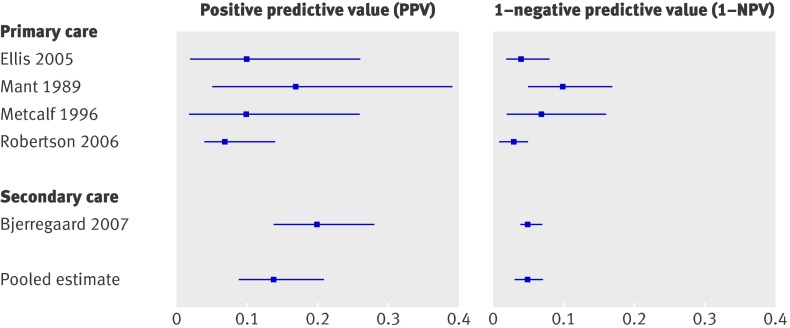
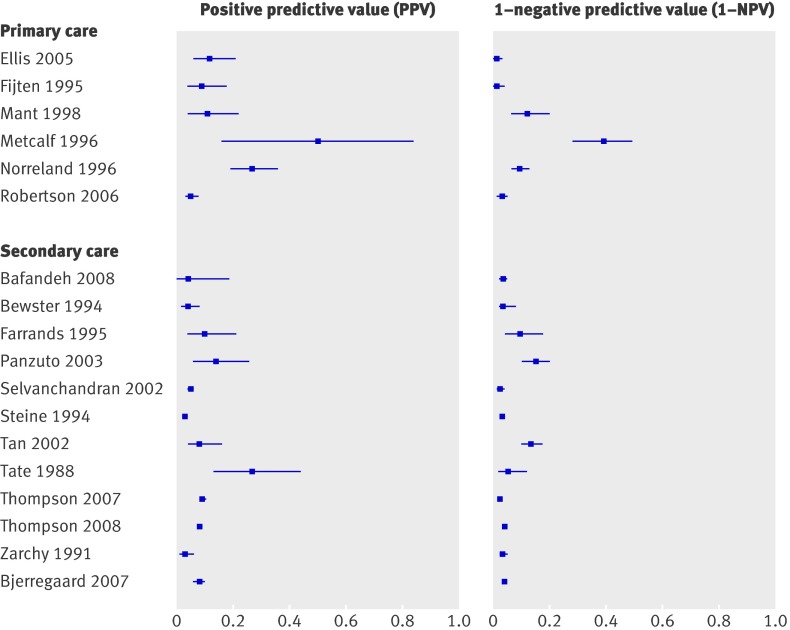
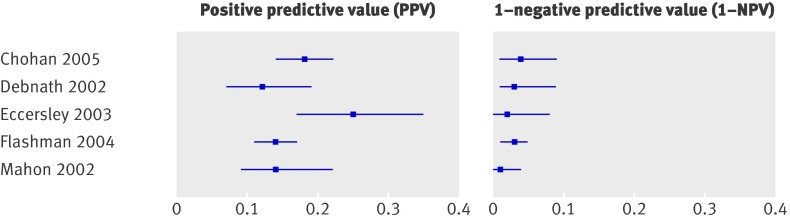
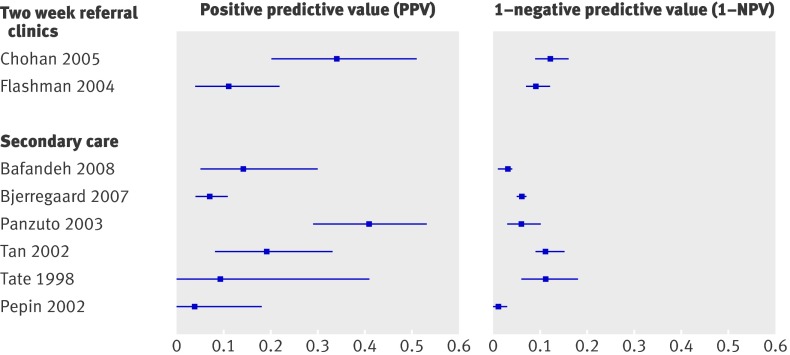
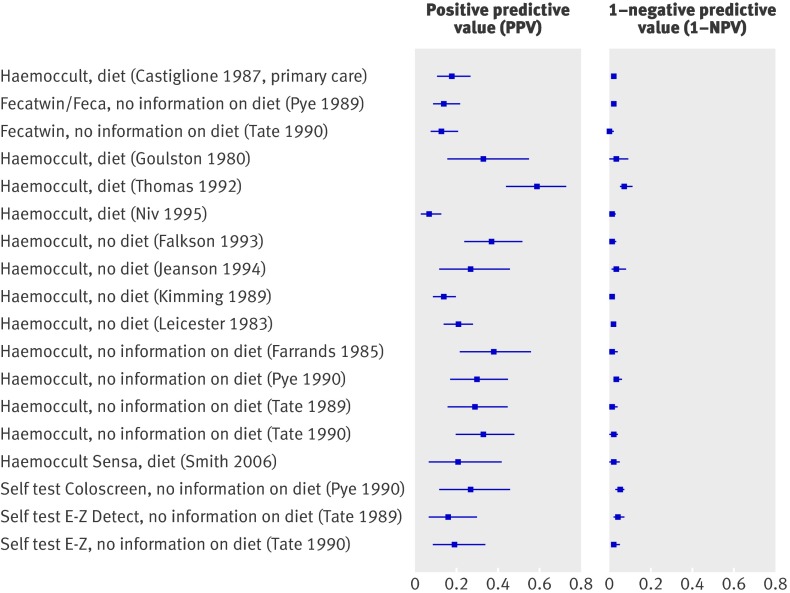
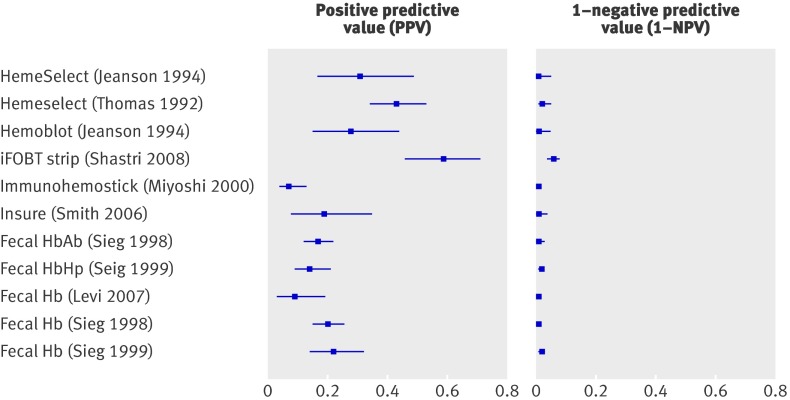
Results: 47 primary diagnostic studies were included. Sensitivity was consistently high for age >or=50 (range 0.81-0.96, median 0.91), a referral guideline (0.80-0.94, 0.92), and immunochemical faeces tests (0.70-1.00, 0.95). Of these, only specificity of the faeces tests was good. Specificity was consistently high for family history (0.75-0.98, 0.91), weight loss (0.72-0.96, 0.89), and iron deficiency anaemia (0.83-0.95, 0.92), but all tests lacked sensitivity. None of these six tests was (sufficiently) studied in primary care.
Conclusions: Although combinations of symptom and results of immunochemical faeces tests showed good diagnostic performance for colorectal cancer, evidence from primary care is lacking. High quality studies on their role in the diagnostic investigation of colorectal cancer in primary care are urgently needed.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Diagnosing colorectal cancer in primary care.BMJ. 2010 Mar 31;340:c1714. doi: 10.1136/bmj.c1714. BMJ. 2010. PMID: 20360222 No abstract available.
-
Colorectal cancer. Secondary care data may mislead.BMJ. 2010 May 11;340:c2503. doi: 10.1136/bmj.c2503. BMJ. 2010. PMID: 20460320 No abstract available.
References
-
- Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P. Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol 2007;18:581-92. - PubMed
-
- Davila RE, Rajan E, Baron TH, Adler DG, Egan JV, Faigel DO, et al. ASGE guideline: colorectal cancer screening and surveillance. Gastrointest Endosc 2006;63:546-57. - PubMed
-
- O’Connell JB, Maggard MA, Ko CY. Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J Natl Cancer Inst 2004;96:140-5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical