

Computed tomographic coronary artery calcium assessment for evaluating chest pain in the emergency department: long-term outcome of a prospective blind study
- PMID: 20360291
- PMCID: PMC2848419
- DOI: 10.4065/mcp.2009.0620
Computed tomographic coronary artery calcium assessment for evaluating chest pain in the emergency department: long-term outcome of a prospective blind study
Abstract
Objective: To determine the long-term outcome of computed tomographic (CT) quantification of coronary artery calcium (CAC) used as a triage tool for patients presenting with chest pain to an emergency department (ED).
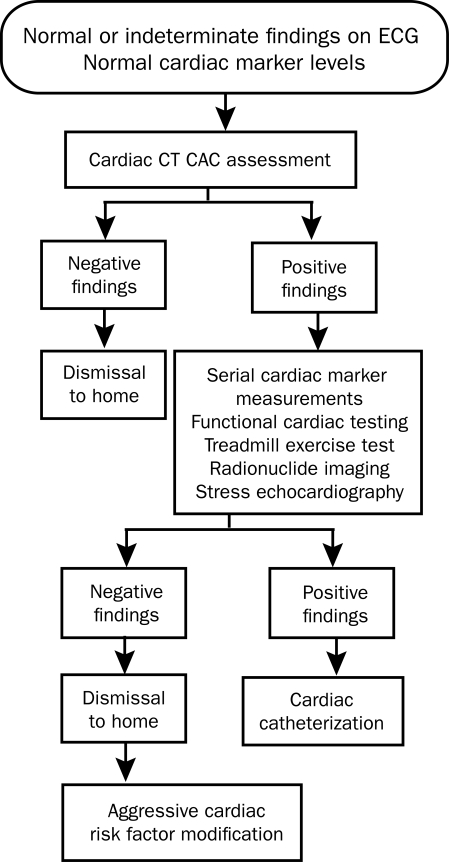
Patients and methods: Patients (men aged 30-62 years and women aged 30-65 years) with chest pain and low-to-moderate probability of coronary artery disease underwent both conventional ED chest pain evaluation and CT CAC assessment prospectively. Patients' physicians were blinded to the CAC results. The results of the conventional evaluation were compared with CAC findings on CT, and the long-term outcome in patients undergoing CT CAC assessment was established. Primary end points (acute coronary syndrome, death, fatal or nonfatal non-ST-segment elevation myocardial infarction, fatal or nonfatal ST-segment elevation myocardial infarction) and secondary outcomes (coronary artery bypass grafting, percutaneous transluminal coronary angioplasty, coronary stenting, or a combination thereof) were obtained when the patient was dismissed from the ED or hospital and then at 30 days, 1 year, and 5 years.
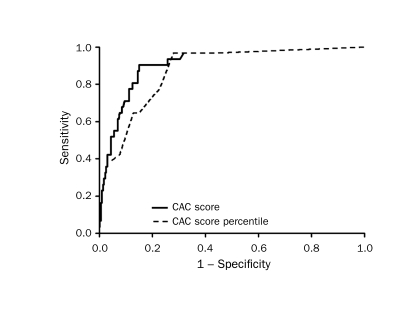
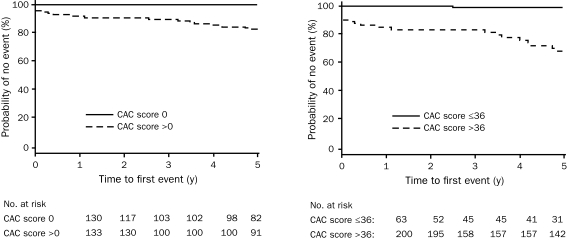
Results: Of the 263 study patients, 133 (51%) had a CAC score of zero. This absence of CAC correlated strongly with the likelihood of noncardiac chest pain. Among 133 patients with a CAC score of zero, only 1 (<1%) had cardiac chest pain. Conversely, of the 31 patients shown to have cardiac chest pain, 30 (97%) had evidence of CAC on CT. When a CAC cutoff score of 36 was used, as suggested by receiver operating characteristic analysis, sensitivity was 90%; specificity, 85%; positive predictive value, 44%; and negative predictive value, 99%. During long-term follow-up, patients without CAC experienced no cardiac events at 30 days, 1 year, and 5 years.
Conclusion: Findings suggest that CT CAC assessment is a powerful adjunct in chest pain evaluation for the population at low-to-intermediate risk. Absent or minimal CAC in this population makes cardiac chest pain extremely unlikely. The absence of CAC suggests an excellent long-term (5-year) prognosis, with no primary or secondary cardiac outcomes occurring in study patients at 5-year follow-up.
Figures
Comment in
-
Emergency department assessment of acute-onset chest pain: contemporary approaches and their consequences.Mayo Clin Proc. 2010 Apr;85(4):309-13. doi: 10.4065/mcp.2010.0141. Mayo Clin Proc. 2010. PMID: 20360290 Free PMC article. No abstract available.
References
-
- Storrow AB, Gibler WB. Chest pain centers: diagnosis of acute coronary syndromes. Ann Emerg Med. 2000;35(5):449-461 - PubMed
-
- Canto JG, Shlipak MG, Rogers WJ, et al. Prevalence, clinical characteristics, and mortality among patients with myocardial infarction presenting without chest pain. JAMA 2000;283(24):3223-3229 - PubMed
-
- Lee TH, Rouan GW, Weisberg MC, et al. Sensitivity of routine clinical criteria for diagnosing myocardial infarction within 24 hours of hospitalization. Ann Intern Med. 1987;106(2):181-186 - PubMed
-
- Gibler WB, Lewis LM, Erb RE, et al. Early detection of acute myocardial infarction in patients presenting with chest pain and nondiagnostic ECGs: serial CK-MB sampling in the emergency department [published correction appears in Ann Emerg Med. 1991;20(4):420] Ann Emerg Med. 1990;19(12):1359-1366 - PubMed
-
- Karras DJ, Kane DL. Serum markers in the emergency department diagnosis of acute myocardial infarction. Emerg Med Clin North Am. 2001;19(2):321-337 - PubMed
