

A "hot" topic in dyslipidemia management--"how to beat a flush": optimizing niacin tolerability to promote long-term treatment adherence and coronary disease prevention
- PMID: 20360295
- PMCID: PMC2848425
- DOI: 10.4065/mcp.2009.0535
A "hot" topic in dyslipidemia management--"how to beat a flush": optimizing niacin tolerability to promote long-term treatment adherence and coronary disease prevention
Abstract
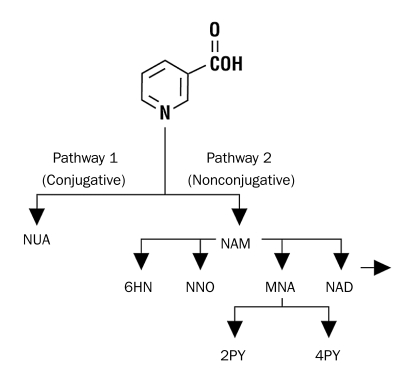
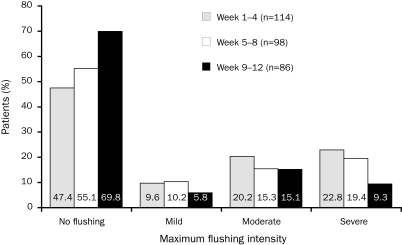
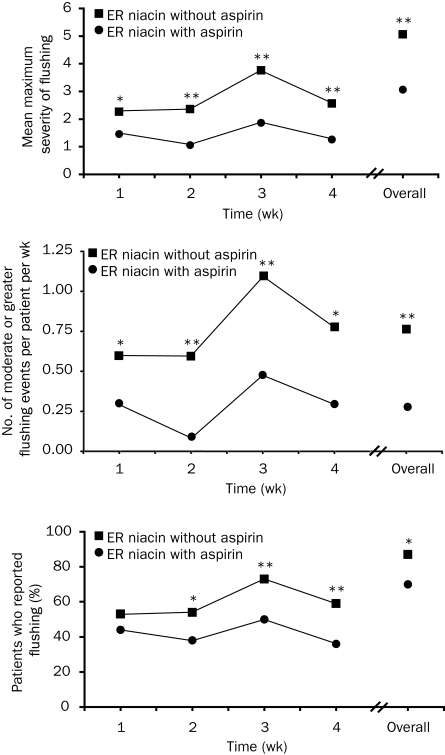
Niacin is the most effective lipid-modifying agent for raising high-density lipoprotein cholesterol levels, but it also causes cutaneous vasodilation with flushing. To determine the frequency of flushing in clinical trials, as well as to delineate counseling and treatment approaches to prevent or manage flushing, a MEDLINE search was conducted of English-language literature from January 1, 1985, through April 7, 2009. This search used the title keywords niacin or nicotinic acid crossed with the Medical Subject Headings adverse effects and human. Niacin flushing is a receptor-mediated, mainly prostaglandin D(2)-driven phenomenon, the frequency, onset, and duration of which are largely determined by the distinct pharmacological and metabolic profiles of different niacin formulations. Subjective assessments include ratings of redness, warmth, itching, and tingling. In clinical trials, most (>60%) niacin users experienced mild or moderate flushing, which tended to decrease in frequency and severity with continued niacin treatment, even with advancing doses. Approximately 5% to 20% of patients discontinued treatment because of flushing. Flushing may be minimized by taking niacin with meals (or at bedtime with a low-fat snack), avoiding exacerbating factors (alcohol or hot beverages), and taking 325 mg of aspirin 30 minutes before niacin dosing. The current review advocates an initially slow niacin dose escalation from 0.5 to 1.0 g/d during 8 weeks and then from 1.0 to 2.0 g in a single titration step (if tolerated). Through effective counseling, treatment prophylaxis with aspirin, and careful dose escalation, adherence to niacin treatment can be improved significantly. Wider implementation of these measures should enable higher proportions of patients to reach sufficient niacin doses over time to prevent cardiovascular events.
Figures
Similar articles
-
Niacin extended-release therapy in phase III clinical trials is associated with relatively low rates of drug discontinuation due to flushing and treatment-related adverse events: a pooled analysis.Am J Cardiovasc Drugs. 2011 Jun 1;11(3):179-87. doi: 10.2165/11592560-000000000-00000. Am J Cardiovasc Drugs. 2011. PMID: 21619381
-
The mechanism and mitigation of niacin-induced flushing.Int J Clin Pract. 2009 Sep;63(9):1369-77. doi: 10.1111/j.1742-1241.2009.02099.x. Int J Clin Pract. 2009. PMID: 19691622 Free PMC article. Review.
-
Extended-release niacin/laropiprant: reducing niacin-induced flushing to better realize the benefit of niacin in improving cardiovascular risk factors.Cardiol Clin. 2008 Nov;26(4):547-60. doi: 10.1016/j.ccl.2008.06.007. Cardiol Clin. 2008. PMID: 19031552 Review.
-
Niacin use and cutaneous flushing: mechanisms and strategies for prevention.Am J Cardiol. 2008 Apr 17;101(8A):14B-19B. doi: 10.1016/j.amjcard.2008.02.028. Am J Cardiol. 2008. PMID: 18375236 Review.
-
Improved control of niacin-induced flushing using an optimized once-daily, extended-release niacin formulation.Int J Clin Pharmacol Ther. 2006 Dec;44(12):633-40. doi: 10.5414/cpp44633. Int J Clin Pharmacol Ther. 2006. PMID: 17190373 Clinical Trial.
Cited by
-
Nicotinic acid activates the capsaicin receptor TRPV1: Potential mechanism for cutaneous flushing.Arterioscler Thromb Vasc Biol. 2014 Jun;34(6):1272-80. doi: 10.1161/ATVBAHA.113.303346. Epub 2014 Mar 27. Arterioscler Thromb Vasc Biol. 2014. PMID: 24675661 Free PMC article.
-
Niacin and biosynthesis of PGD₂by platelet COX-1 in mice and humans.J Clin Invest. 2012 Apr;122(4):1459-68. doi: 10.1172/JCI59262. Epub 2012 Mar 12. J Clin Invest. 2012. PMID: 22406532 Free PMC article. Clinical Trial.
-
The Role of GPR109a Signaling in Niacin Induced Effects on Fed and Fasted Hepatic Metabolism.Int J Mol Sci. 2021 Apr 13;22(8):4001. doi: 10.3390/ijms22084001. Int J Mol Sci. 2021. PMID: 33924461 Free PMC article.
-
Stress triggers coronary mast cells leading to cardiac events.Ann Allergy Asthma Immunol. 2014 Apr;112(4):309-16. doi: 10.1016/j.anai.2013.09.017. Epub 2013 Oct 10. Ann Allergy Asthma Immunol. 2014. PMID: 24428962 Free PMC article. Review.
-
Cardiodermatology: the heart of the connection between the skin and cardiovascular disease.Nat Rev Cardiol. 2025 May;22(5):354-371. doi: 10.1038/s41569-024-01097-9. Epub 2024 Nov 13. Nat Rev Cardiol. 2025. PMID: 39537837 Review.
References
-
- Adult Treatment Panel Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106(25):3143-3421 - PubMed
-
- Graham I, Atar D, Borch-Johnsen K, et al. European guidelines on cardiovascular disease prevention in clinical practice: full text. Fourth Joint Task Force of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of nine societies and by invited experts). Eur J Cardiovasc Prev Rehabil. 2007;14(Suppl 2):S1-S113 - PubMed
-
- Hausenloy DJ, Yellon DM. Targeting residual cardiovascular risk: raising high-density lipoprotein cholesterol levels. Heart 2008;94(6):706-714 - PubMed
-
- Altschul R, Hoffer A, Stephen JD. Influence of nicotinic acid on serum cholesterol in man. Arch Biochem. 1955;54(2):558-559 - PubMed
-
- Canner PL, Berge KG, Wenger NK, et al. Fifteen year mortality in Coronary Drug Project patients: long-term benefit with niacin. J Am Coll Cardiol. 986;8(6):1245-1255 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
