

Review
doi: 10.3174/ajnr.A2043.
Epub 2010 Apr 1.
The present and the future of neuroimaging in amyotrophic lateral sclerosis
Affiliations
- PMID: 20360339
- PMCID: PMC7964007
- DOI: 10.3174/ajnr.A2043
Item in Clipboard
Review
The present and the future of neuroimaging in amyotrophic lateral sclerosis
AJNR Am J Neuroradiol.
2010 Nov.
Abstract
In patients with ALS, conventional MR imaging is frequently noninformative, and its use has been restricted to excluding other conditions that can mimic ALS. Conversely, the extensive application of modern MR imaging-based techniques to the study of ALS has undoubtedly improved our understanding of disease pathophysiology and is likely to have a role in the identification of potential biomarkers of disease progression. This review summarizes how new MR imaging technology is changing dramatically our understanding of the factors associated with ALS evolution and highlights the reasons why it should be used more extensively in studies of disease progression, including clinical trials.
Figures
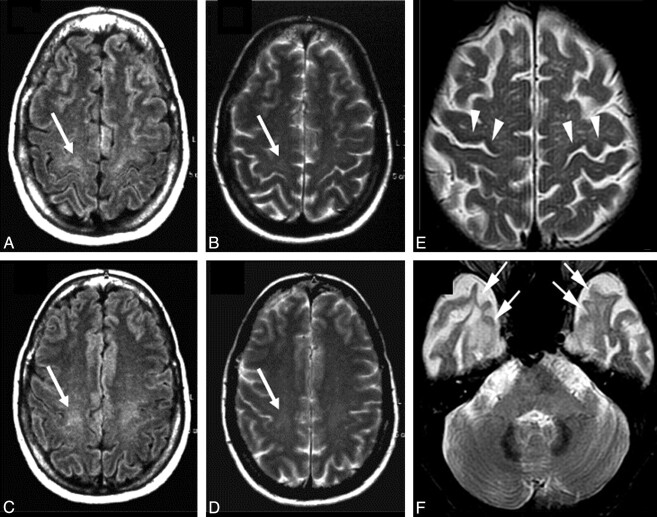
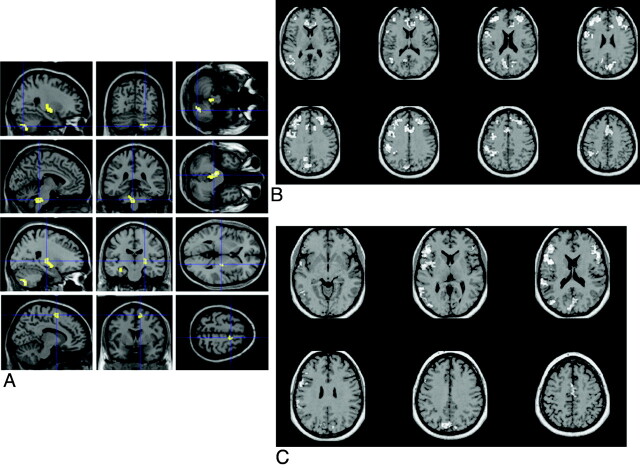
Conventional MR imaging findings in patients with ALS. A−D, Hyperintensity at the subcortical precentral gyrus (A and B) and the centrum semiovale (C and D) on FLAIR (arrows, A and C) and T2-weighted (arrows, B and D) images of a 66-year-old patient with ALS. Modified with permission from Hecht et al.
E and F, T2-weighted images obtained from a 58-year-old patient with ALS with dementia show hypointensity along the precentral cortices (arrowheads, E) and symmetric hyperintensity in the anterior temporal subcortical WM (arrows, F). A and D reprinted with permission from the Journal of the Neurological Sciences (2001;186:37–44). Copyright 2001, Elsevier Ltd.
Regional GM atrophy in patients with ALS compared with controls. A group comparison of 17 patients with ALS versus 17 healthy controls shows regional GM atrophy in the precentral and postcentral gyri bilaterally, which extends from the primary motor cortex to the premotor, parietal, and frontal regions bilaterally (displayed at P = .001, uncorrected; extended threshold, 100 voxels). The color bar represents the t-score. The differences between groups are superimposed on a standard normalized T1-weighted image. Images are shown in neurologic convention.
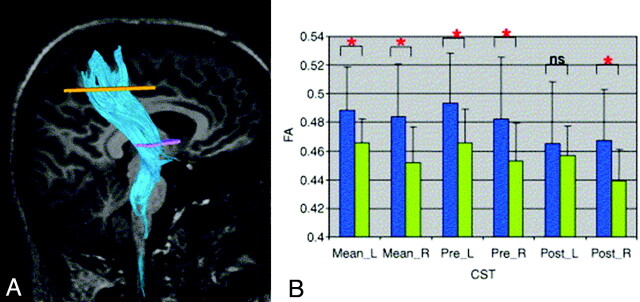
A, A representative example of DTI tractography of the CST. B, Graphs of mean FA in the right and left CSTs of 28 patients with ALS (green) and 26 healthy controls (blue). Data are presented for the entire CST (mean) and its pre- and postcentral portions. Mean values are shown with SDs (black lines). Significant differences in diffusion parameters between groups are indicated by a red asterisk. Reprinted with permission from Neuroimage (2007;34:486–99). Copyright 2007, Elsevier Ltd.
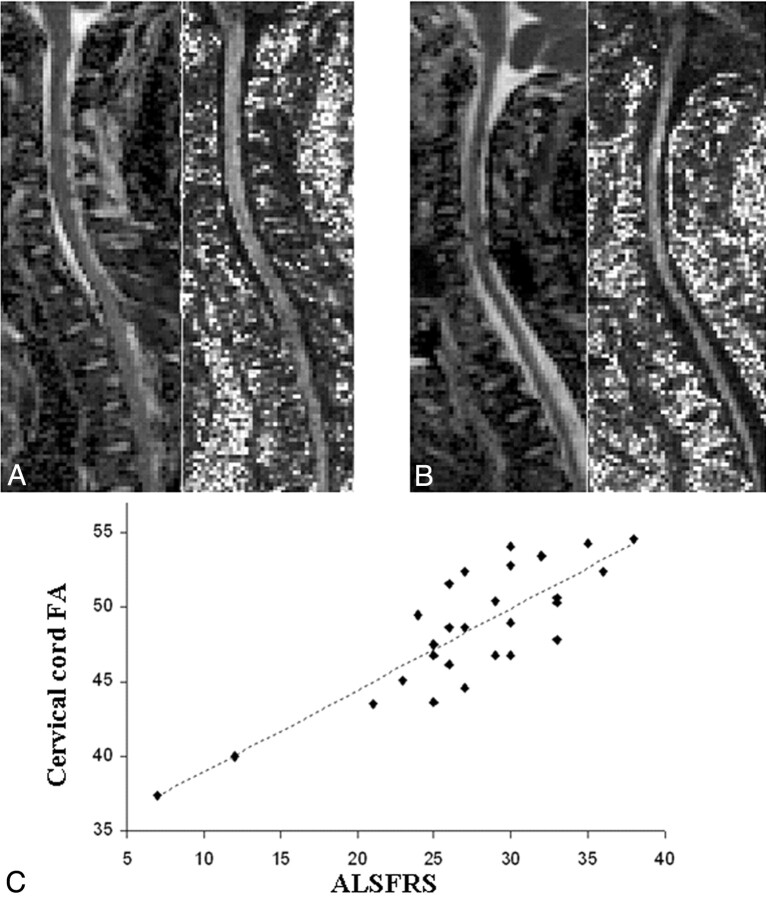
A and B, Illustrative examples of MD (images on the left of each pair) and FA (images on the right of each pair) maps of the cervical cord obtained from a healthy volunteer (A) and a patient with ALS (B). C, Scatterplot of the correlation between the cervical cord FA and the ALSFRS in 28 patients with ALS. Reprinted with permission from the Journal of Neurology, Neurosurgery & Psychiatry (2007;78:480–84). Copyright 2007, BMJ Publishing Group Ltd.
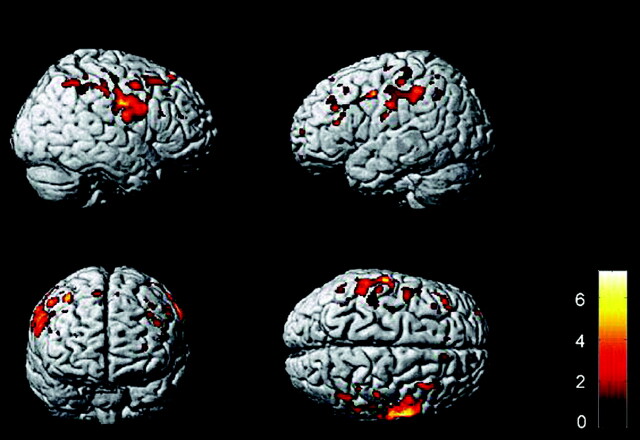
A, Brain regions showing a significant increased recruitment on fMRI scans from 10 patients with ALS relative to 10 healthy controls during right-handed movement (P < .05, small volume correction). Modified with permission from Konrad et al.
B and C, Areas of reduced fMRI activation in 28 nondemented patients with ALS relative to the control group during letter fluency (B) and confrontation naming (C) tasks. A reprinted with permission from Experimental Brain Research (2006;172:361–69). Copyright 2006, Springer Science + Business Media. B and C reprinted with permission from Brain (2004;127:1507–17). Copyright 2004, Oxford University Press.
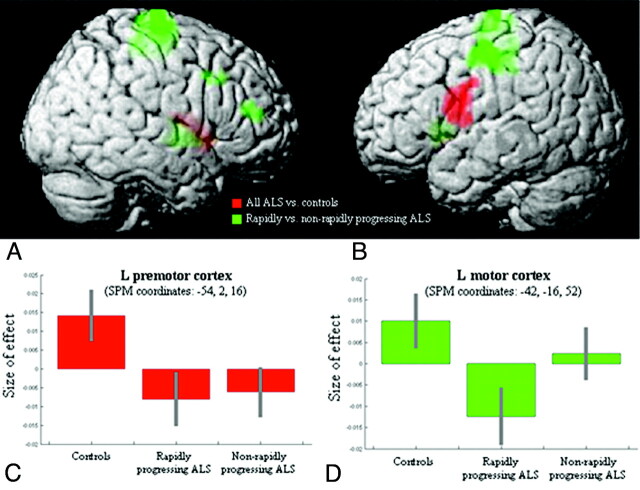
Regions showing progression of GM atrophy during a 9-month period in 16 patients with ALS compared with 10 controls (red) and regions showing additional GM loss in clinically rapidly progressing patients with ALS compared with both controls and nonrapidly progressing patients (green). A and B, Results are superimposed on the 3D rendering of the Montreal Neurologic Institute standard brain and displayed at a threshold of P < .05, uncorrected. Color saturation depends on the position of the brain region in relation to the cortical surface in the rendered brain (ie, motor, premotor, and prefrontal regions are more saturated; basal ganglia are less saturated). C and D, Plots showing the “size of effect” in the left premotor and motor cortices for each group of subjects (healthy controls, patients with rapidly progressing ALS, and those with nonrapidly progressing ALS). The “size of the effect” was obtained by plotting the estimates of the analysis of variance model parameters, which were of interest in the present analysis (3 subject groups). The bars represent the 90% confidence intervals. Reprinted with permission from Amyotrophic Lateral Sclerosis (2009;10:168–74). Copyright 2009, Taylor and Francis.
References
-
- Dion PA, Daoud H, Rouleau GA. Genetics of motor neuron disorders: new insights into pathogenic mechanisms. Nat Rev Genet 2009;10:769–82 - PubMed
-
- Neumann M, Sampathu DM, Kwong LK, et al. Ubiquitinated TDP-43 in frontotemporal lobar degeneration and amyotrophic lateral sclerosis. Science 2006;314:130–33 - PubMed
-
- Andersen PM, Borasio GD, Dengler R, et al. EFNS task force on management of amyotrophic lateral sclerosis: guidelines for diagnosing and clinical care of patients and relatives. Eur J Neurol 2005;12:921–38 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous