

The triple rule-out for acute ischemic stroke: imaging the brain, carotid arteries, aorta, and heart
- PMID: 20360341
- PMCID: PMC7965468
- DOI: 10.3174/ajnr.A2075
The triple rule-out for acute ischemic stroke: imaging the brain, carotid arteries, aorta, and heart
Abstract
Background and purpose: Ischemic stroke is commonly embolic, either from carotid atherosclerosis or from cardiac origin. These potential sources of emboli need to be investigated to accurately prescribe secondary stroke prevention. Moreover, the mortality in ischemic stroke patients due to ischemic heart disease is greater than that of age-matched controls, thus making evaluation for coronary artery disease important in this patient population. The purpose of this study was to evaluate the image quality of a comprehensive CTA protocol in patients with acute stroke that expands the standard CTA coverage to include all 4 chambers of the heart and the coronary arteries.
Materials and methods: One hundred twenty patients consecutively admitted to the emergency department with suspected cerebrovascular ischemia undergoing standard-of-care CTA were prospectively enrolled in our study. We used an original tailored acquisition protocol using a 64-section CT scanner, consisting of a dual-phase intravenous injection of iodinated contrast and saline flush, in conjunction with a dual-phase CT acquisition, ascending from the top of the aortic arch to the vertex of the head, then descending from the top of the aortic arch to the diaphragm. No beta blockers were administered. The image quality, attenuation, and CNRs of the carotid, aortic, vertebral, and coronary arteries were assessed.
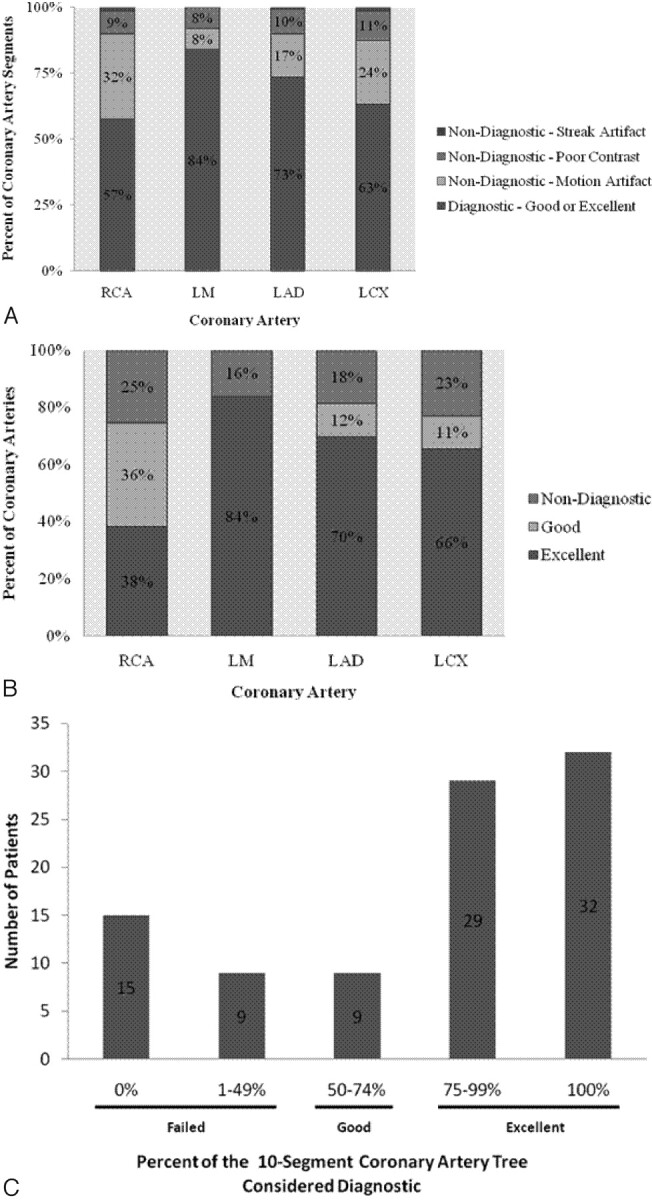
Results: Carotid, aorta, and vertebral artery image quality was 100% diagnostic (rated good or excellent) in all patients. Coronary artery image quality was diagnostic in 58% of RCA segments, 73% of LAD segments, and 63% of LCX segments. When we considered proximal segments only, the diagnostic quality rose to 71% in the RCA, 83% in the LAD, and 74% in the LCX.
Conclusions: Our stroke protocol achieved excellent opacification of the left heart chambers, the cervical arteries, and each coronary artery, in addition to adequate carotid and coronary artery image quality.
Figures


References
-
- Adams HP, Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke: definitions for use in a multicenter clinical trial—TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993;24:35–41 - PubMed
-
- Wintermark M, Flanders AE, Velthuis B, et al. Perfusion-CT assessment of infarct core and penumbra: receiver operating characteristic curve analysis in 130 patients suspected of acute hemispheric stroke. Stroke 2006;37:979–85 - PubMed
-
- Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease—the American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke 2009;40:2276–93. Epub 2009 May 7 - PubMed
-
- de Bruijn SF, Agema WR, Lammers GJ, et al. Transesophageal echocardiography is superior to transthoracic echocardiography in management of patients of any age with transient ischemic attack or stroke. Stroke 2006;37:2531–34 - PubMed
-
- Hur J, Kim YJ, Lee HJ, et al. Cardiac computed tomographic angiography for detection of cardiac sources of embolism in stroke patients. Stroke 2009;40:2073–78 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical