

Intracranial stent placement for recanalization of acute cerebrovascular occlusion in 32 patients
- PMID: 20360342
- PMCID: PMC7965458
- DOI: 10.3174/ajnr.A2055
Intracranial stent placement for recanalization of acute cerebrovascular occlusion in 32 patients
Abstract
Background and purpose: Stents have been reported as an option for improvement of the recanalization rate in AIS. The authors have also used intracranial stents in failed cases of IAT with pharmacologic and mechanical methods since 2004. We retrospectively reviewed our cases of intracranial stent use for IAT of AIS for recanalization and as a rescue procedure for iatrogenic intracranial vascular dissection during IAT.
Materials and methods: Thirty-two patients, who were diagnosed with AIS, were treated with intracranial stents (28 balloon-mounted and 7 self-expandable stents) at our neurovascular center between April 2004 and December 2008. The stent use for all 32 patients was the final attempt to recanalize occluded vessels after various trials of pharmacologic or mechanical thrombolysis or to treat iatrogenic vascular dissection.
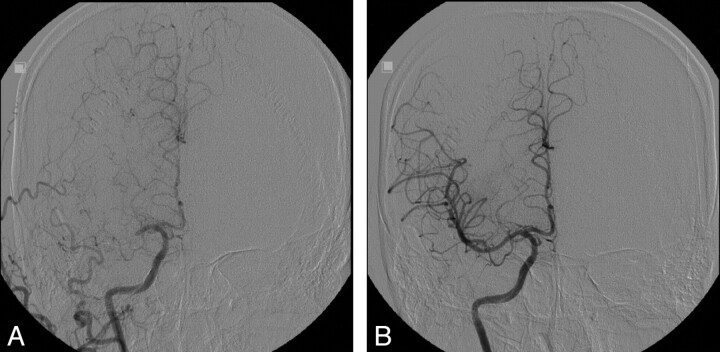
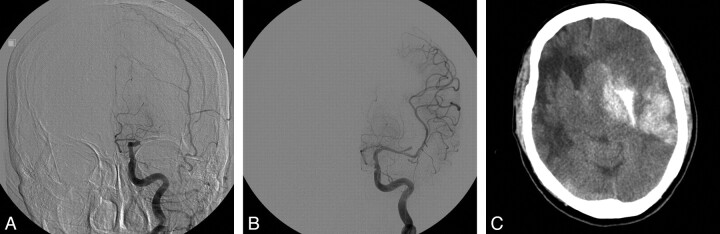
Results: Among the 32 patients, immediate poststenting angiographic recanalization was achieved in 100% with TIMI/TICI 2 (15 of 32 lesions, 46.9%) or TIMI/TICI 3 (17 of 32 lesions, 53.1%). However, complication rates were also high. Major symptomatic intracerebral hemorrhage (1 case of procedural symptomatic hemorrhage and 3 cases of delayed symptomatic hemorrhage) occurred in 4 (12.5%); intracranial vascular dissection, in 4 (12.5%); extracranial vascular dissection, in 3 (9.4%); immediate IST, in 4 (12.5%); subacute (within 1 week) IST, in 2; late (>1 week) IST, in 1, and 1 case of in-stent restenosis occurred twice (at 5 and 17 months).
Conclusions: Intracranial stent placement for AIS management has an excellent recanalization rate. However, it is associated with high complication risks as our series showed. We believe that the decision to treat AIS with intracranial stent placement should be made after careful consideration of potential benefits and risks.
Figures
References
-
- Tissue plasminogen activator for acute ischemic stroke: The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med 1995;333:1581–87 - PubMed
-
- Furlan A, Higashida R, Wechsler L, et al. Intra-arterial prourokinase for acute ischemic stroke: The PROACT II study—a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA 1999;282:2003–11 - PubMed
-
- Gobin YP, Starkman S, Duckwiler GR, et al. MERCI 1: a phase 1 study of Mechanical Embolus Removal in Cerebral Ischemia. Stroke 2004;35:2848–54. Epub 2004 Oct 28 - PubMed
-
- Smith WS, Sung G, Starkman S, et al. Safety and efficacy of mechanical embolectomy in acute ischemic stroke: results of the MERCI trial. Stroke 2005;36:1432–38 - PubMed
-
- Smith WS, Sung G, Saver J, et al. Mechanical thrombectomy for acute ischemic stroke: final results of the Multi MERCI trial. Stroke 2008;39:1205–12 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous