

Cellular assessment of muscle in COPD: case studies of two males
- PMID: 20360908
- PMCID: PMC2840564
- DOI: 10.2147/ijgm.s5981
Cellular assessment of muscle in COPD: case studies of two males
Abstract
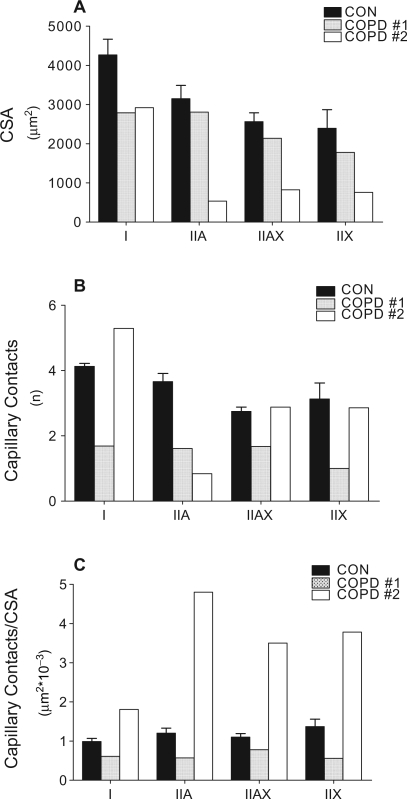
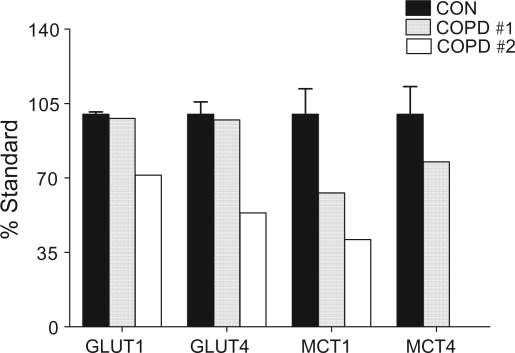
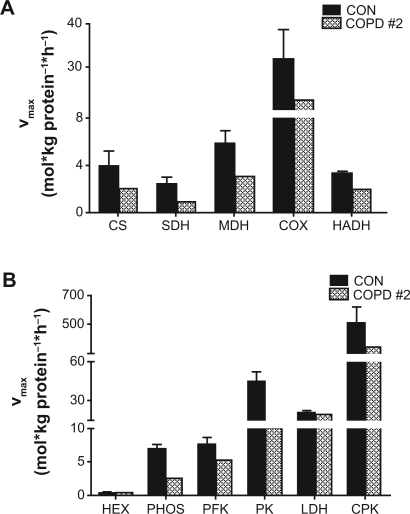
The objective of this paper is to provide an overview of the recent developments in muscle physiology and biochemistry in general, and with respect to chronic obstructive pulmonary disease (COPD) specifically. As a way of illustration, we have presented data on the remodeling that occurs in vastus lateralis in two patients with COPD (COPD #1, forced expiratory volume in one second/forced vital capacity [FEV(1)/FVC] = 63%; COPD #2, FEV(1)/FVC = 41%) exhibiting differences in muscle wasting as compared to healthy controls (CON; FEV(1)/FVC = 111 +/- 2.2%, n = 4). Type I fibers percentages were lower in both COPD #1 (16.7) and COPD #2 (24.9) compared to CON (57.3 +/- 5.2). Cross sectional area of the type I fibers of the patients ranged between 65%-68% of CON and for the type II subtypes (IIA, IIAX, IIX) between 74% and 89% (COPD #1) and 17%-32% (COPD #2). A lower number of capillary contacts were observed for all fiber types in COPD #1 but not COPD #2. Lower concentrations of adenosine triphosphate (ATP) (24%-26%) and phosphocreatine (18%-20%), but not lactate occurred in COPD. In contrast to COPD #1, who displayed normal glucose transporter content, GLUT1 and GLUT4 were only 71% and 54%, respectively of CON in COPD #2. Lower monocarboxylate contents were found for MCT1 in both COPD #1 (63%) and COPD #2 (41%) and for MCT4 (78%) in COPD #1. Maximal oxidative enzyme activities (V(max)) for COPD #2 ranged between 37% (succinic dehydrogenase) and 70% (cytochrome C oxidase) of CON. For the cytosolic enzymes, V(max) ranged between 89% (hexokinase) to 31% (pyruvate kinase) of CON. Depressions were also observed in V(max) of the Na(+)-K(+)-ATPase for COPD #1 (66% of CON) but not COPD #2 (92% of CON) while V(max) of the Ca(2+)-ATPase was near normal in COPD #1 (84% CON). It is concluded that disturbances can occur in muscle to a wide range of excitation, contraction and metabolic processes in COPD.
Keywords: area; capillarization; enzymatic pathways; excitation-contraction processes; fiber types; glucose and monocarboxylate transporters; metabolism; vastus lateralis.
Figures
Similar articles
-
Muscle fiber type characteristics in females with chronic obstructive pulmonary disease. A preliminary study.J Mol Histol. 2009 Feb;40(1):41-51. doi: 10.1007/s10735-009-9211-8. Epub 2009 Feb 11. J Mol Histol. 2009. PMID: 19205906
-
Organization of metabolic pathways in vastus lateralis of patients with chronic obstructive pulmonary disease.Am J Physiol Regul Integr Comp Physiol. 2008 Sep;295(3):R935-41. doi: 10.1152/ajpregu.00167.2008. Epub 2008 Jul 16. Am J Physiol Regul Integr Comp Physiol. 2008. PMID: 18635455
-
Altered metabolic and transporter characteristics of vastus lateralis in chronic obstructive pulmonary disease.J Appl Physiol (1985). 2008 Sep;105(3):879-86. doi: 10.1152/japplphysiol.90458.2008. Epub 2008 Jul 17. J Appl Physiol (1985). 2008. PMID: 18635880
-
Abnormal sarcoplasmic reticulum Ca2+-sequestering properties in skeletal muscle in chronic obstructive pulmonary disease.Am J Physiol Cell Physiol. 2008 Aug;295(2):C350-7. doi: 10.1152/ajpcell.00224.2008. Epub 2008 May 28. Am J Physiol Cell Physiol. 2008. PMID: 18508908
-
Tiotropium bromide. A review of its use as maintenance therapy in patients with COPD.Treat Respir Med. 2004;3(4):247-68. doi: 10.2165/00151829-200403040-00005. Treat Respir Med. 2004. PMID: 15350163 Review.
References
-
- Hamilton AL, Killian KJ, Summers E, Jones NL. Muscle strength, symptom intensity and exercise capacity in patients with cardiorespiratory disorders. Am J Respir Critical Care Med. 1995;152:2021–2031. - PubMed
-
- Gosker HR, Wouters EF, van der Vusse GJ, Schols AM. Skeletal muscle dysfunction in chronic obstructive pulmonary disease and chronic heart failure: underlying mechanisms and therapy perspectives. Am J Clin Nutr. 2000;71:1033–1047. - PubMed
-
- Troosters T, Gosselink R, Decramer M. Chronic obstructive pulmonary disease and chronic heart failure. J Cardiopul Rehab. 2004;24:137–145. - PubMed
-
- Green HJ, Burnett TA, Duhamel TA, et al. Abnormal sarcoplasmic reticulum Ca2+-sequestering properties in skeletal muscle in chronic obstructive lung disease. Am J Physiol. 2008;295:C350–C357. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
