

Improving child protection in the emergency department: a systematic review of professional interventions for health care providers
- PMID: 20370740
- PMCID: PMC3023813
- DOI: 10.1111/j.1553-2712.2009.00640.x
Improving child protection in the emergency department: a systematic review of professional interventions for health care providers
Abstract
Objectives: This systematic review evaluated the effectiveness of professional and organizational interventions aimed at improving medical processes, such as documentation or clinical assessments by health care providers, in the care of pediatric emergency department (ED) patients where abuse was suspected.
Methods: A search of electronic databases, references, key journals, and conference proceedings was conducted and primary authors were contacted. Studies whose purpose was to evaluate a strategy aimed at improving ED clinical care of suspected abuse were included. Study methodologic quality was assessed by two independent reviewers. One reviewer extracted the data, and a second checked for completeness and accuracy.
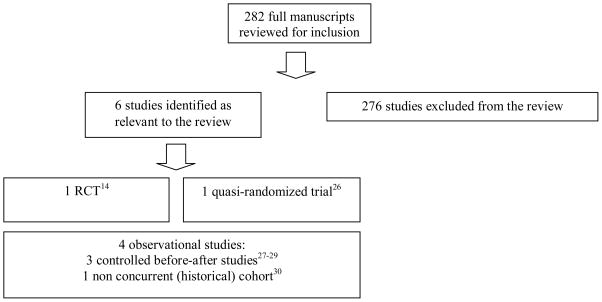
Results: Six studies met the inclusion criteria: one randomized controlled trial (RCT), one quasi-RCT, and four observational studies. Study quality ranged from modest (observational studies) to good (trials). Variation in study interventions and outcomes limited between-study comparisons. The quasi-RCT supported self-instructional education kits as a means to improve physician knowledge for both physical abuse (mean +/- standard deviation [SD] pretest score = 13.12 +/- 2.36; mean +/- SD posttest score = 18.16 +/- 1.64) and sexual abuse (mean +/- SD pretest score = 10.81 +/- 3.20; mean +/- SD posttest score = 18.45 +/- 1.79). Modest-quality observational studies evaluated reminder systems for physician documentation with similar results across studies. Compared to standard practice, chart checklists paired with an educational program increased physician consideration of nonaccidental burns in burn cases (59% increase), documentation of time of injury (36% increase), and documentation of consistency (53% increase) and compatibility (55% increase) of reported histories. Decisional flow charts for suspected physical abuse also increased documentation of nonaccidental physical injury (69.5% increase; p < 0.0001) and had a similar significant effect as checklists on increasing documentation of history consistency and compatibility (69.5 and 70.0% increases, respectively; p < 0.0001) when compared to standard practice. No improvements were noted in these studies for documentation of consultations or current status with child protective services. The introduction of a specialized team and crisis center to standardize practice had little effect on physician documentation, but did increase documentation of child protective services involvement (22.7% increase; p < 0.005) and discharge status (23.7% increase; p < 0.02). Referral to social services increased in one study following the introduction of a chart checklist (8.6% increase; p = 0.018). A recently conducted multisite RCT did not support observational findings, reporting no significant effect of educational sessions and/or a chart checklist on ED practices.
Conclusions: The small number of studies identified in this review highlights the need for future quality studies that address care of a vulnerable clinical population. While moderate-quality observational studies suggest that education and reminder systems increase clinical knowledge and documentation, these findings are not supported by a multisite randomized trial. The limited theoretical base for conceptualizing change in health care providers and the influence of the ED environment on clinical practice are limitations to this current evidence base.
(c) 2010 by the Society for Academic Emergency Medicine.
Similar articles
-
Interventions for patients and caregivers to improve knowledge of sickle cell disease and recognition of its related complications.Cochrane Database Syst Rev. 2016 Oct 6;10(10):CD011175. doi: 10.1002/14651858.CD011175.pub2. Cochrane Database Syst Rev. 2016. PMID: 27711980 Free PMC article.
-
Interventions for preventing abuse in the elderly.Cochrane Database Syst Rev. 2016 Aug 16;2016(8):CD010321. doi: 10.1002/14651858.CD010321.pub2. Cochrane Database Syst Rev. 2016. PMID: 27528431 Free PMC article.
-
Nutritional interventions for survivors of childhood cancer.Cochrane Database Syst Rev. 2016 Aug 22;2016(8):CD009678. doi: 10.1002/14651858.CD009678.pub2. Cochrane Database Syst Rev. 2016. PMID: 27545902 Free PMC article.
-
Education support services for improving school engagement and academic performance of children and adolescents with a chronic health condition.Cochrane Database Syst Rev. 2023 Feb 8;2(2):CD011538. doi: 10.1002/14651858.CD011538.pub2. Cochrane Database Syst Rev. 2023. PMID: 36752365 Free PMC article.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
Cited by
-
Developing the Geriatric Injury Documentation Tool (Geri-IDT) to Improve Documentation of Physical Findings in Injured Older Adults.J Gen Intern Med. 2019 Apr;34(4):567-574. doi: 10.1007/s11606-019-04844-8. Epub 2019 Feb 13. J Gen Intern Med. 2019. PMID: 30761452 Free PMC article.
-
Evaluation of a multisite educational intervention to improve mobilization of older patients in hospital: protocol for mobilization of vulnerable elders in Ontario (MOVE ON).Implement Sci. 2013 Jul 3;8:76. doi: 10.1186/1748-5908-8-76. Implement Sci. 2013. PMID: 23822563 Free PMC article.
-
Finding the Victim of Abuse: A New Frontier of Physicians' Liability? Data From a Local Italian Experience on Minor Maltreatment.Front Pediatr. 2020 Jun 19;8:309. doi: 10.3389/fped.2020.00309. eCollection 2020. Front Pediatr. 2020. PMID: 32637388 Free PMC article.
-
Educational paper: Detection of child abuse and neglect at the emergency room.Eur J Pediatr. 2012 Jun;171(6):877-85. doi: 10.1007/s00431-011-1551-1. Epub 2011 Sep 1. Eur J Pediatr. 2012. PMID: 21881926 Free PMC article. Review.
-
The Value of a Checklist for Child Abuse in Out-of-Hours Primary Care: To Screen or Not to Screen.PLoS One. 2017 Jan 3;12(1):e0165641. doi: 10.1371/journal.pone.0165641. eCollection 2017. PLoS One. 2017. PMID: 28045904 Free PMC article.
References
-
- U.S. Department of Health and Human Services, Administration on Children, Youth and Families. Child Maltreatment 2006. Washington, DC: U.S. Government Printing Office; 2008.
-
- Trocmé N, Fallon B, MacLaurin B, Daciuk J, Felstiner C, Black T, Tonmyr L, et al. Canadian Incidence Study of Reported Child Abuse and Neglect – 2003: Major Findings. Ottawa, ON: Minister of Public Works and Government Services Canada; 2005.
-
- Jack S, Munn C, Cheng C, MacMillan H for the National Clearinghouse on Family Violence. Child Maltreatment in Canada: Overview Paper. Ottawa, ON: Public Health Agency of Canada; 2006.
-
- MacMillan HL, Jamieson E, Walsh CA. Repeated contact with child protection services among those reporting child physical and sexual abuse: Results from a community survey. Child Abuse & Neglect. 2003;27(1):1397–1408. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
