

Validation of length of hospital stay as a surrogate measure for injury severity and resource use among injury survivors
- PMID: 20370743
- PMCID: PMC4715859
- DOI: 10.1111/j.1553-2712.2009.00647.x
Validation of length of hospital stay as a surrogate measure for injury severity and resource use among injury survivors
Abstract
Objectives: While hospital length of stay (LOS) has been used as a surrogate injury outcome when more detailed outcomes are unavailable, it has not been validated. This project sought to validate LOS as a proxy measure of injury severity and resource use in heterogeneous injury populations.
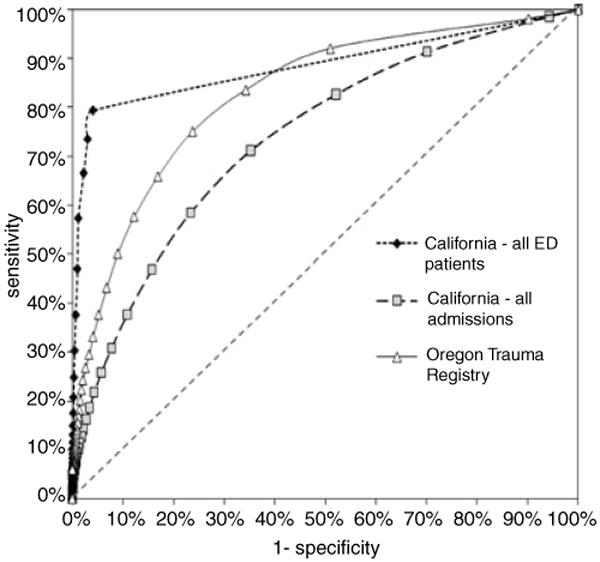
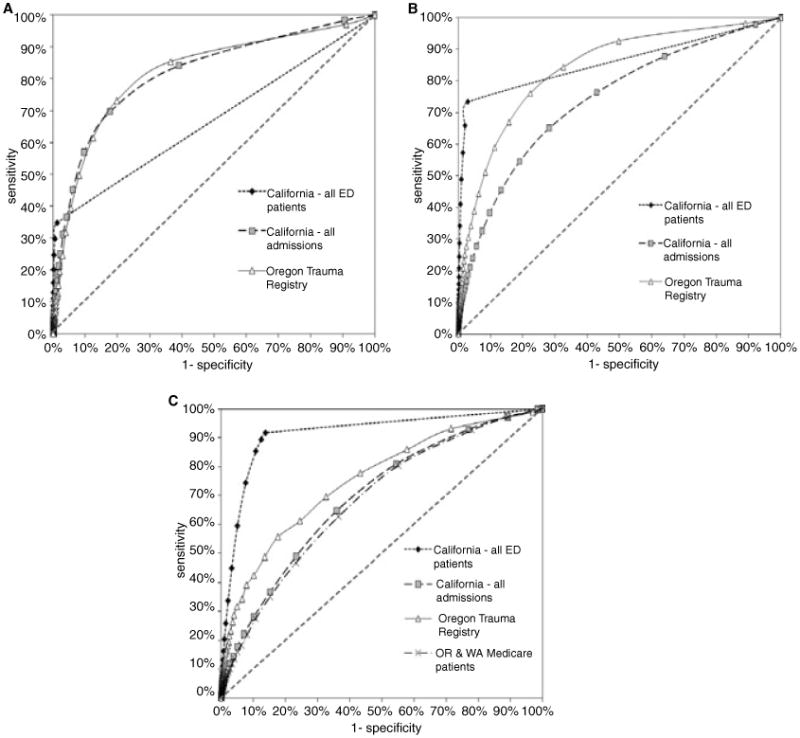
Methods: This observational study used four retrospective cohorts: patients presenting to 339 California emergency departments (EDs) with a primary International Classification of Diseases, Ninth Revision (ICD-9), injury diagnosis (years 2005-2006); California hospital injury admissions (a subset of the ED population); trauma patients presenting to 48 Oregon EDs (years 1998-2003); and injured Medicare patients admitted to 171 Oregon and Washington hospitals (years 2001-2002). In-hospital deaths were excluded, as they represent adverse outcomes regardless of LOS. Duration of hospital stay was defined as the number of days from ED admission to hospital discharge. The primary composite outcome (dichotomous) was serious injury (Injury Severity Score [ISS] >or= 16 or ICD-9 ISS <or= 0.90) or resource use (major surgery, blood transfusion, or prolonged ventilation). The discriminatory accuracy of LOS for identifying the composite outcome was evaluated using receiver operating characteristic (ROC) analysis. Analyses were also stratified by age (0-14, 15-64, and >or=65 years), hospital type, and hospital annual admission volume.
Results: The four cohorts included 3,989,409 California ED injury visits (including admissions), 236,639 California injury admissions, 23,817 Oregon trauma patients, and 30,804 Medicare injury admissions. Composite outcome rates for the four cohorts were 2.1%, 29%, 27%, and 22%, respectively. Areas under the ROC curves for overall LOS were 0.88 (California ED), 0.74 (California admissions), 0.82 (Oregon trauma patients), and 0.68 (Medicare patients). In general, the discriminatory value of LOS was highest among children, tertiary trauma centers, and higher volume hospitals, although this finding differed by the injury population and outcome assessed.
Conclusions: Hospital LOS may be a reasonable proxy for serious injury and resource use among injury survivors when more detailed outcomes are unavailable, although the discriminatory value differs by age and the injury population being studied.
(c) 2010 by the Society for Academic Emergency Medicine.
Figures
References
-
- Committee on the Future of Emergency Care in the United States Health System, Board on Health Care Services Future of Emergency Care Series: Emergency Medical Services, At the Crossroads Institute of Medicine of the National Academies. Washington, DC: The National Academies Press; 2006.
-
- Keim SM, Spaite DW, Maio RF, et al. Establishing the scope and methodological approach to out-of-hospital outcomes and effectiveness research. Ann Emerg Med. 2004;11:1067–73. - PubMed
-
- McLean SA, Maio RF, Spaite DW, Garrison HG. Emergency medical services outcomes research: evaluating the effectiveness of prehospital care. Prehosp Emerg Care. 2002;6(2 Suppl):S52–6. - PubMed
-
- Maio RF, Garrison HG, Spaite DW, et al. Emergency medical services outcomes project I (EMSOP I): prioritizing conditions for outcomes research. Ann Emerg Med. 1999;33:423–32. - PubMed
-
- Spaite DW, Maio R, Garrison HG, et al. Emergency medical services outcomes project (EMSOP) II: developing the foundation and conceptual models for out-of-hospital outcomes research. Ann Emerg Med. 2001;37:657–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
