

Deep posterior compartment strength and foot kinematics in subjects with stage II posterior tibial tendon dysfunction
- PMID: 20371019
- PMCID: PMC2871386
- DOI: 10.3113/FAI.2010.0320
Deep posterior compartment strength and foot kinematics in subjects with stage II posterior tibial tendon dysfunction
Abstract
Background: Tibialis posterior muscle weakness has been documented in subjects with Stage II posterior tibial tendon dysfunction (PTTD) but the effect of weakness on foot structure remains unclear. The association between strength and flatfoot kinematics may guide treatment such as the use of strengthening programs targeting the tibialis posterior muscle.
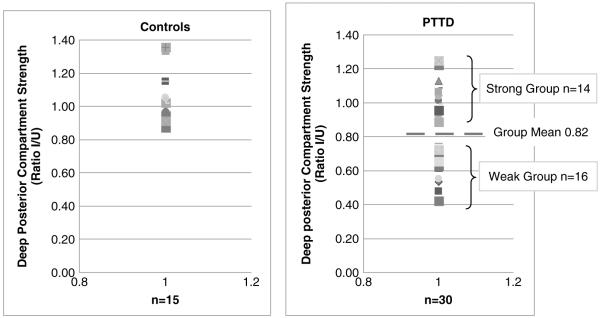
Materials and methods: Thirty Stage II PTTD subjects (age; 58.1 +/- 10.5 years, BMI 30.6 +/- 5.4) and 15 matched controls (age; 56.5 +/- 7.7 years, BMI 30.6 +/- 3.6) volunteered for this study. Deep Posterior Compartment strength was measured from both legs of each subject and the strength ratio was used to compare each subject's involved side to their uninvolved side. A 20% deficit was defined, a priori, to define two groups of subjects with PTTD. The strength ratio for each group averaged; 1.06 +/- 0.1 (range 0.87 to 1.36) for controls, 1.06 +/- 0.1 (range, 0.89 to 1.25), for the PTTD strong group, and 0.64 +/- 0.2 (range 0.42 to 0.76) for the PTTD weak group. Across four phases of stance, kinematic measures of flatfoot were compared between the three groups using a two-way mixed effect ANOVA model repeated for each kinematic variable.
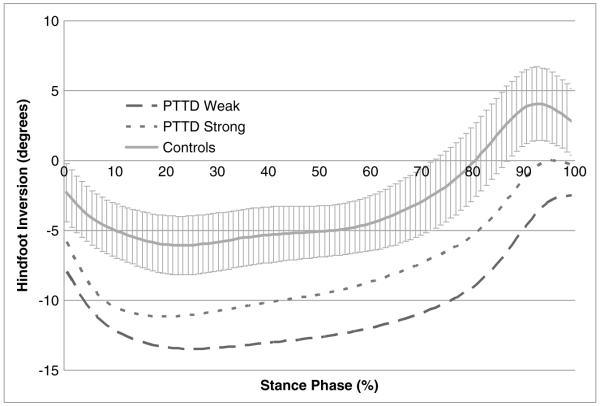
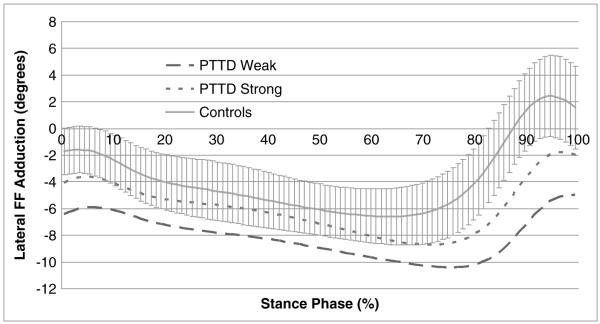
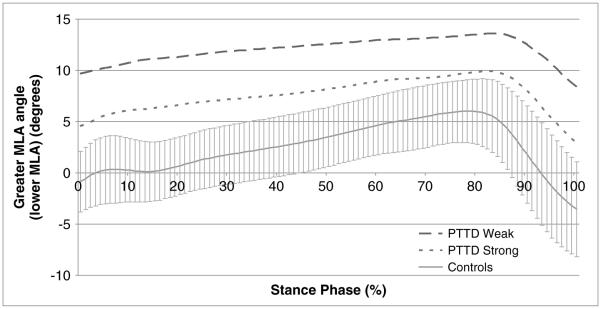
Results: Subjects with PTTD regardless of group demonstrated significantly greater hindfoot eversion compared to controls. Subjects with PTTD who were weak demonstrated greater hindfoot eversion compared to subjects with PTTD who were strong. For forefoot abduction and MLA angles the differences between groups depended on the phase of stance with significant differences between each group observed at the pre-swing phase of stance.
Conclusion: Strength was associated with the degree of flatfoot deformity observed during walking, however, flatfoot deformity may also occur without strength deficits.
Clinical relevance: Strengthening programs may only partially correct flatfoot kinematics while other clinical interventions such as bracing or surgery may also be indicated.
Figures
References
-
- Alvarez RG, Marini A, Schmitt C, Saltzman CL. Stage I and II Posterior Tibial Tendon Dysfunction Treated by a Structured Nonoperative Management Protocol: An Orthosis and Exercise Program. Foot Ankle Int. 2006;26(9):671–4. 27 2 - 8. - PubMed
-
- Arai K, Ringleb SI, Zhao KD, et al. The effect of flatfoot deformity and tendon loading on the work of friction measured in the posterior tibial tendon. Clinical Biomechanics. 2007;22:592–598. http://dx.doi.org/10.1016/j.clinbiomech.2007.01.011. - DOI - PubMed
-
- Bluman EM, Title CI, Myerson MS. Posterior Tibial Tendon Rupture: A Refined Classification System. Foot and ankle clinics. 2007;12:233. http://dx.doi.org/10.1016/j.fcl.2007.03.003. - DOI - PubMed
-
- Browning RC, Baker EA, Herron JA, Kram R. Effects of obesity and sex on the energetic cost and preferred speed of walking. J. Appl. Physiol. 2006;100:390–398. http://dx.doi.org/10.1152/japplphysiol.00767.2005. - DOI - PubMed
-
- Cole GK, Nigg BM, Ronsky JL, Yeadon MR. Application of the joint coordinate system to three-dimensional joint attitude and movement representation: a standardization proposal. J. Biomech. Eng. 1993;115:344–349. http://dx.doi.org/10.1115/1.2895496. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
