

Uncovering residual effects of chronic sleep loss on human performance
- PMID: 20371466
- PMCID: PMC2892834
- DOI: 10.1126/scitranslmed.3000458
Uncovering residual effects of chronic sleep loss on human performance
Abstract
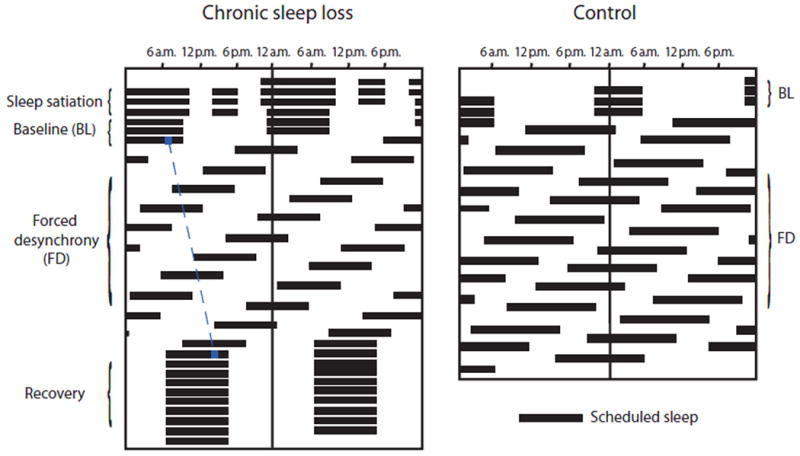
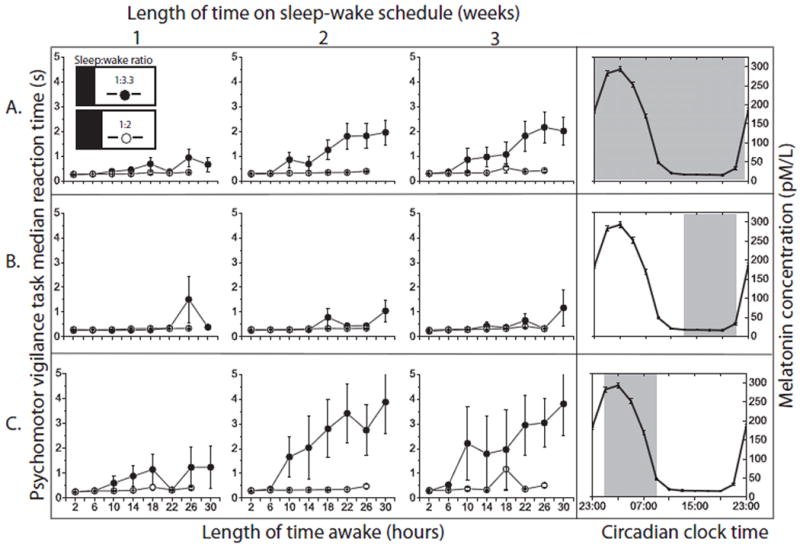
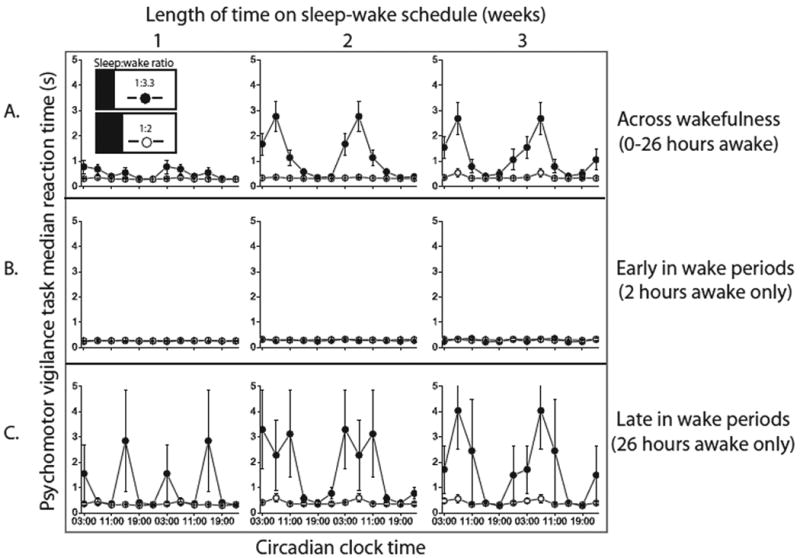
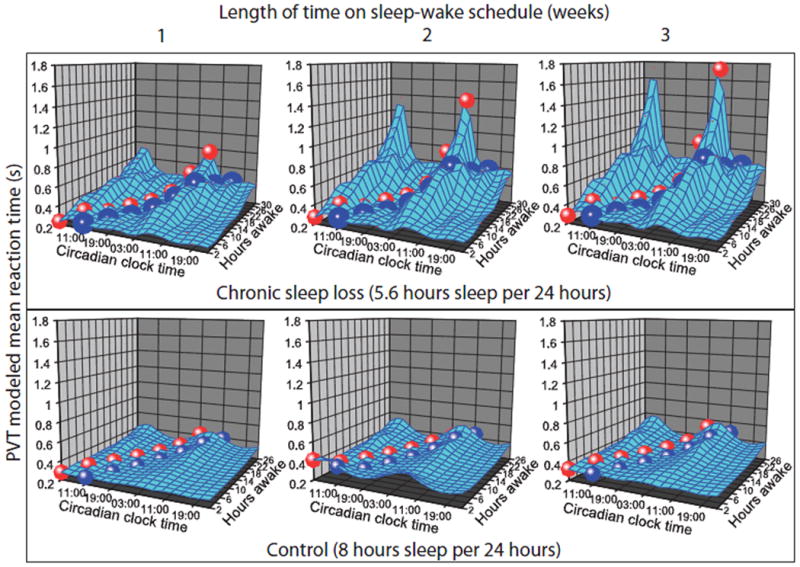
Sleep loss leads to profound performance decrements. Yet many individuals believe they adapt to chronic sleep loss or that recovery requires only a single extended sleep episode. To evaluate this, we designed a protocol whereby the durations of sleep and wake episodes were increased to 10 and 32.85 hours, respectively, to yield a reduced sleep-to-wake ratio of 1:3.3. These sleep and wake episodes were distributed across all circadian phases, enabling measurement of the effects of acute and chronic sleep loss at different times of the circadian day and night. Despite recurrent acute and substantial chronic sleep loss, 10-hour sleep opportunities consistently restored vigilance task performance during the first several hours of wakefulness. However, chronic sleep loss markedly increased the rate of deterioration in performance across wakefulness, particularly during the circadian "night." Thus, extended wake during the circadian night reveals the cumulative detrimental effects of chronic sleep loss on performance, with potential adverse health and safety consequences.
Figures
References
-
- Van Dongen HPA, Maislin G, Mullington JM, Dinges DF. The cumulative cost of additional wakefulness: Dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Sleep. 2003;26:117–126. - PubMed
-
- Klein DC, Moore RY, Reppert SM. Suprachiasmatic nucleus: The mind's clock. Oxford University Press; New York: 1991.
-
- Dijk DJ, Czeisler CA. Paradoxical timing of the circadian rhythm of sleep propensity serves to consolidate sleep and wakefulness in humans. Neurosci Lett. 1994;166:63–68. - PubMed
-
- Deboer T, Detari L, Meijer JH. Long term effects of sleep deprivation on the mammalian circadian pacemaker. Sleep. 2007;30:257–262. - PubMed
-
- Dijk DJ, Duffy JF, Czeisler CA. Circadian and sleep/wake dependent aspects of subjective alertness and cognitive performance. J Sleep Res. 1992;1:112–117. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
