

Inducing CTLA-4-dependent immune regulation by selective CD28 blockade promotes regulatory T cells in organ transplantation
- PMID: 20371478
- PMCID: PMC2860737
- DOI: 10.1126/scitranslmed.3000116
Inducing CTLA-4-dependent immune regulation by selective CD28 blockade promotes regulatory T cells in organ transplantation
Abstract
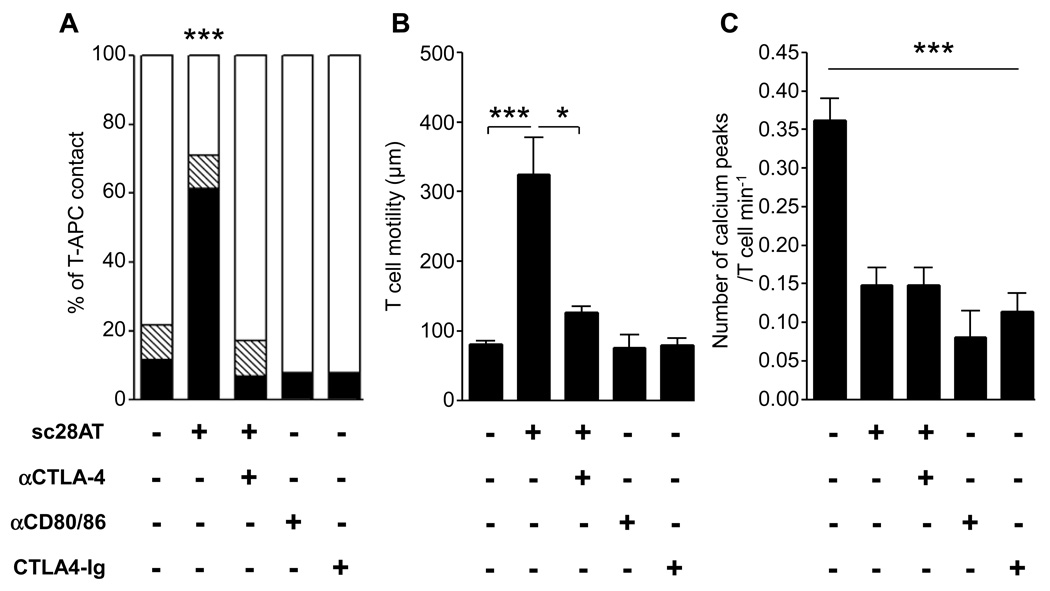
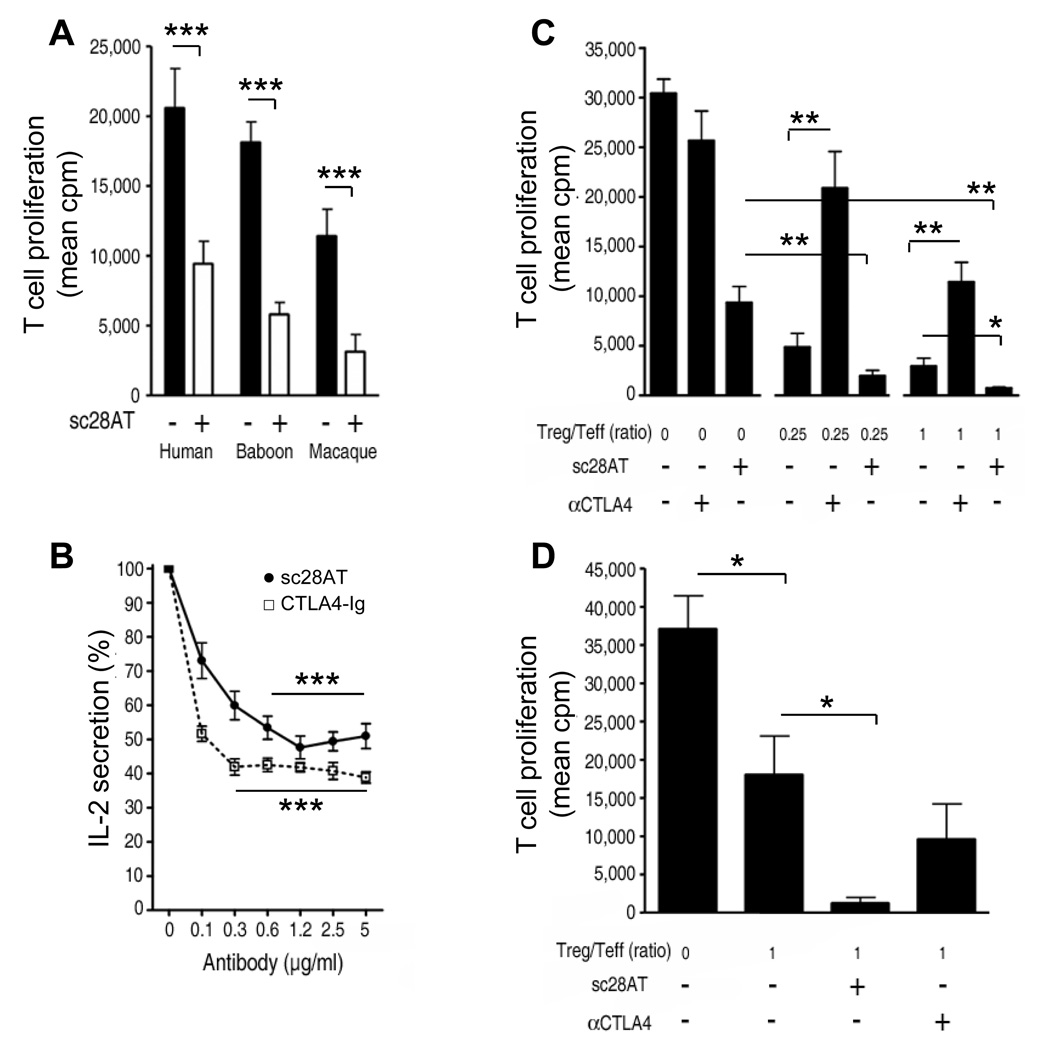
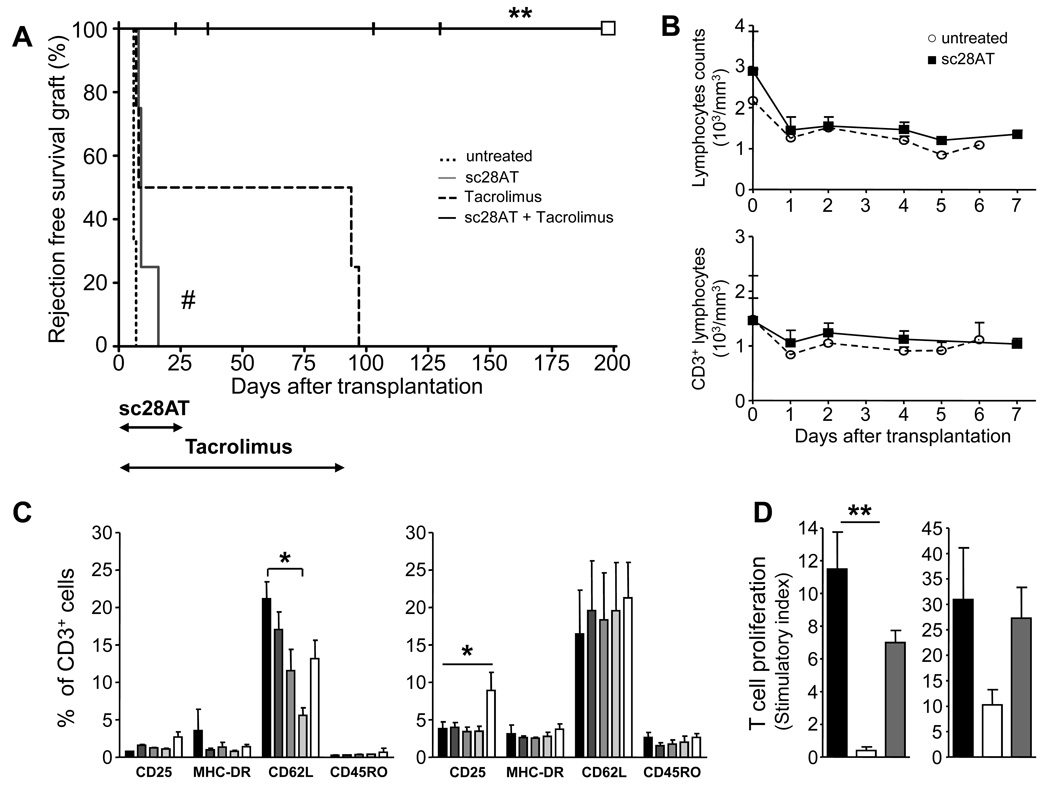
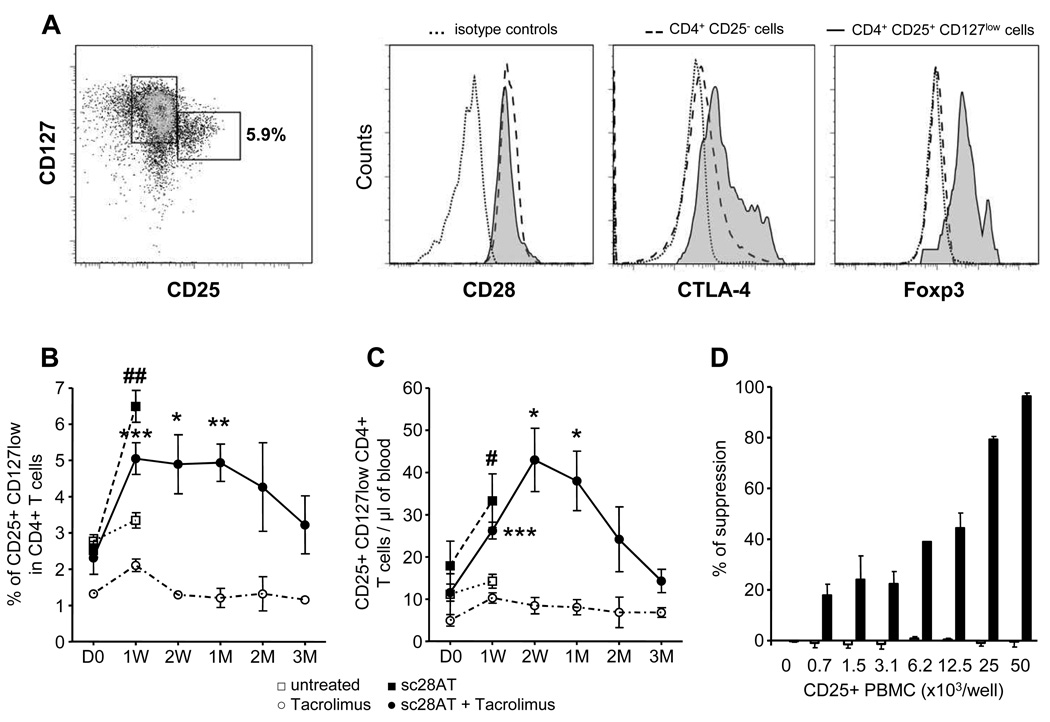
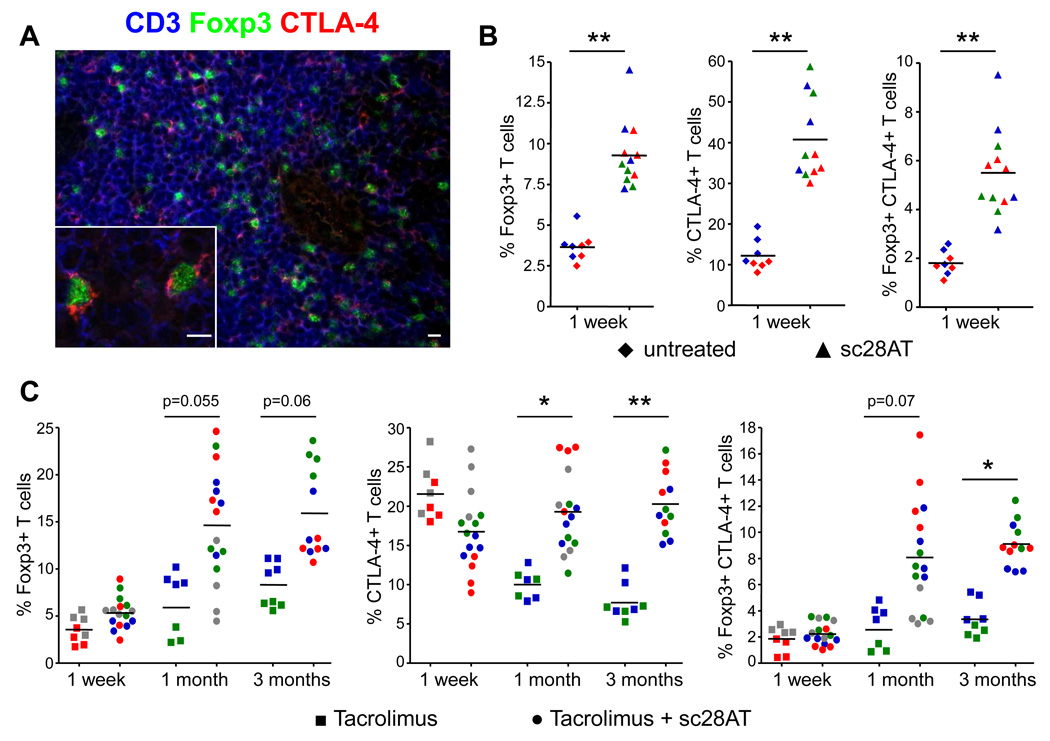
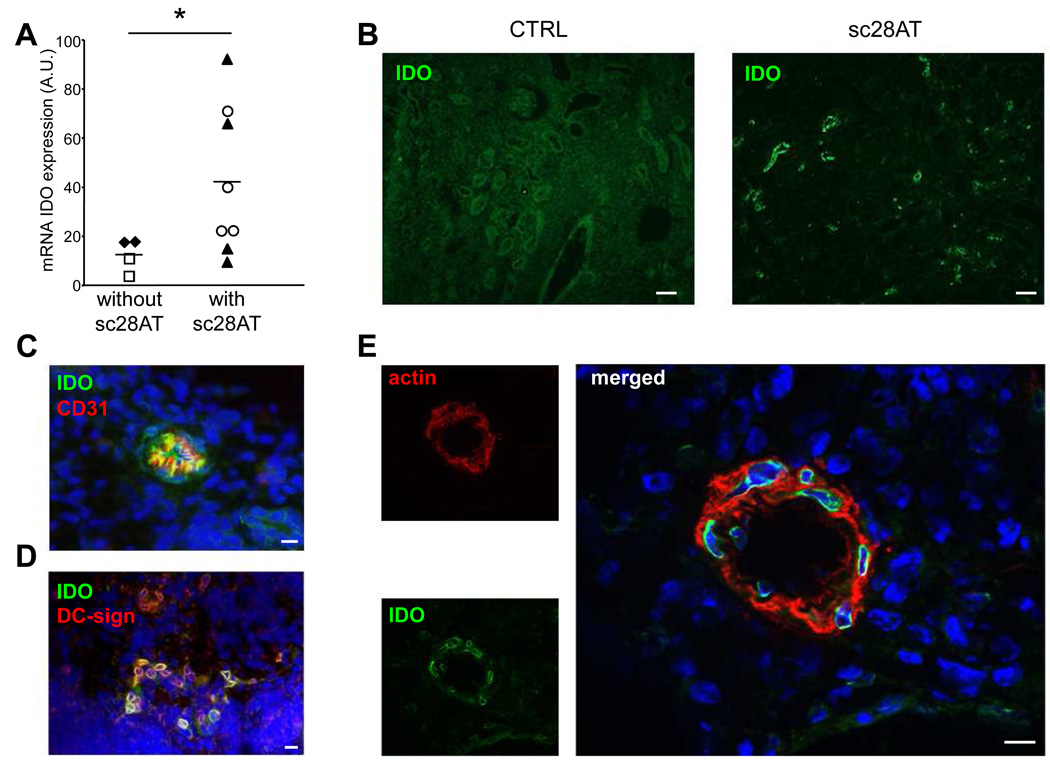
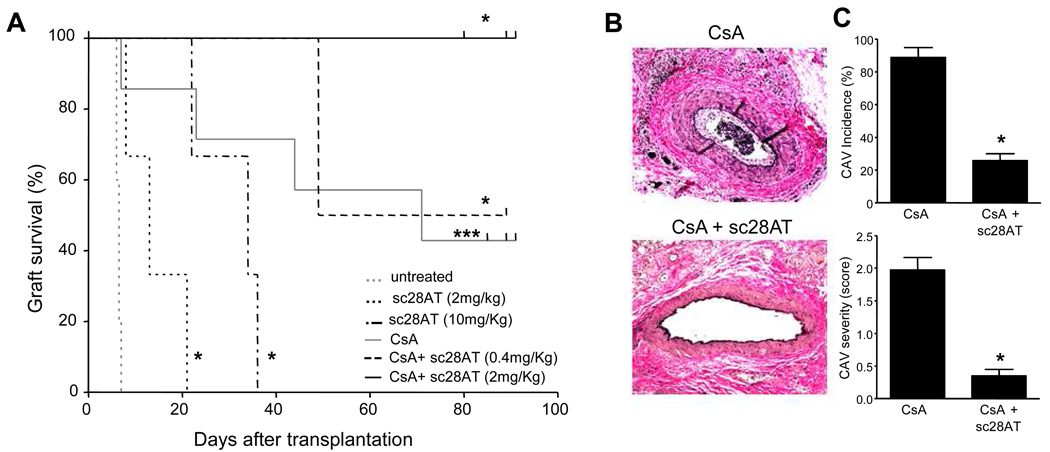
Transplantation is the treatment of choice for patients with end-stage organ failure. Its success is limited by side effects of immunosuppressive drugs, such as inhibitors of the calcineurin pathway that prevent rejection by reducing synthesis of interleukin-2 by T cells. Moreover, none of the existing drugs efficiently prevent the eventual rejection of the organ. Blocking the CD28-mediated T cell costimulation pathway is a nontoxic alternative immunosuppression strategy that is now achieved by blockade of CD80/86, the receptor for CD28 on antigen-presenting cells. However, interaction of CD80/86 with cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) is required for immune regulation. Therefore, CD28 blockade, instead of CD80/86 blockade, might preserve regulatory signals mediated by CTLA-4 and preserve immune regulation. By using monovalent antibodies, we identified true CD28 antagonists that induced CTLA-4-dependent decreased T cell function compatible with regulatory T (Treg) cell suppression. In transplantation experiments in primates, blocking CD28 augmented intragraft and peripheral blood Treg cells, induced molecular signatures of immune regulation, and prevented graft rejection and vasculopathy in synergy with calcineurin inhibition. These findings suggest that targeting costimulation blockade at CD28 preserves CTLA-4-dependent immune regulation and promotes allograft survival.
Figures
References
-
- Alegre ML, Frauwirth KA, Thompson CB. T-cell regulation by CD28 and CTLA-4. Nat Rev Immunol. 2001;1:220–228. - PubMed
-
- Kremer JM, Westhovens R, Leon M, Di Giorgio E, Alten R, Steinfeld S, Russell A, Dougados M, Emery P, Nuamah IF, Williams GR, Becker JC, Hagerty DT, Moreland LW. Treatment of rheumatoid arthritis by selective inhibition of T-cell activation with fusion protein CTLA4Ig. N Engl J Med. 2003;349:1907–1915. - PubMed
-
- Vincenti F, Larsen C, Durrbach A, Wekerle T, Nashan B, Blancho G, Lang P, Grinyo J, Halloran PF, Solez K, Hagerty D, Levy E, Zhou W, Natarajan K, Charpentier B. Costimulation blockade with belatacept in renal transplantation. N Engl J Med. 2005;353:770–781. - PubMed
-
- Takahashi T, Kuniyasu Y, Toda M, Sakaguchi N, Itoh M, Iwata M, Shimizu J, Sakaguchi S. Immunologic self-tolerance maintained by CD25+CD4+ naturally anergic and suppressive T cells: induction of autoimmune disease by breaking their anergic/suppressive state. Int Immunol. 1998;10:1969–1980. - PubMed
-
- Salomon B, Lenschow DJ, Rhee L, Ashourian N, Singh B, Sharpe A, Bluestone JA. B7/CD28 costimulation is essential for the homeostasis of the CD4+CD25+ immunoregulatory T cells that control autoimmune diabetes. Immunity. 2000;12:431–440. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
