

Phase I/II study of inhaled doxorubicin combined with platinum-based therapy for advanced non-small cell lung cancer
- PMID: 20371682
- PMCID: PMC4262532
- DOI: 10.1158/1078-0432.CCR-09-3015
Phase I/II study of inhaled doxorubicin combined with platinum-based therapy for advanced non-small cell lung cancer
Abstract
Purpose: We have shown the feasibility of administering inhaled doxorubicin to patients with cancer. This study evaluated inhaled doxorubicin combined with cisplatin and docetaxel in patients with non-small cell lung cancer. The principal objective was to determine safety and, secondarily, efficacy.
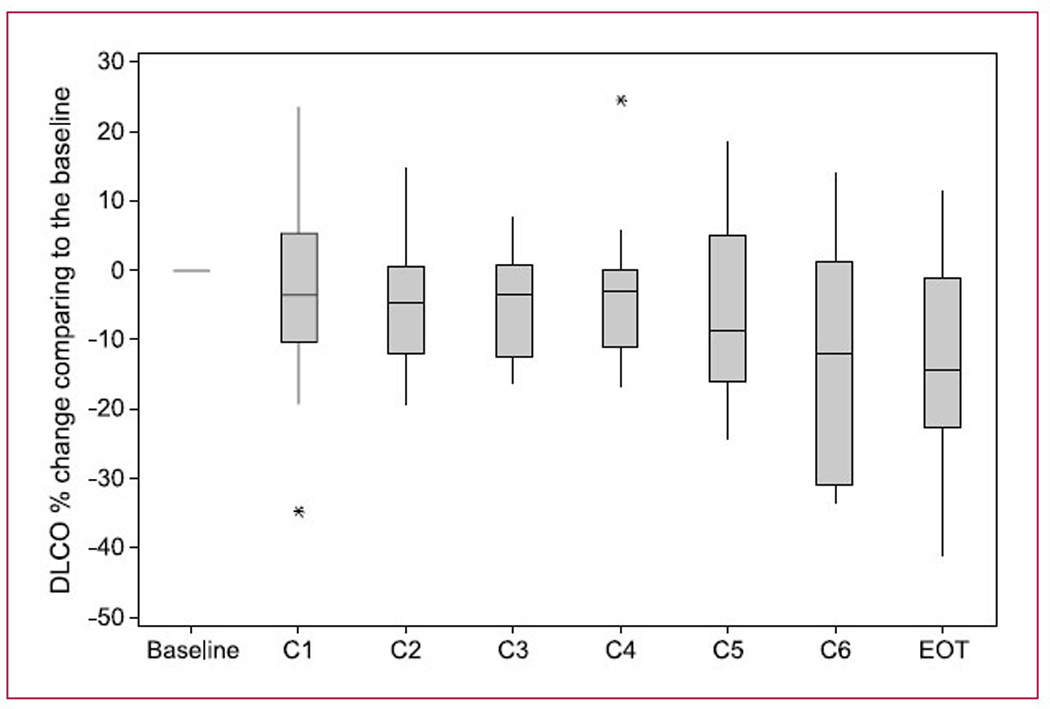
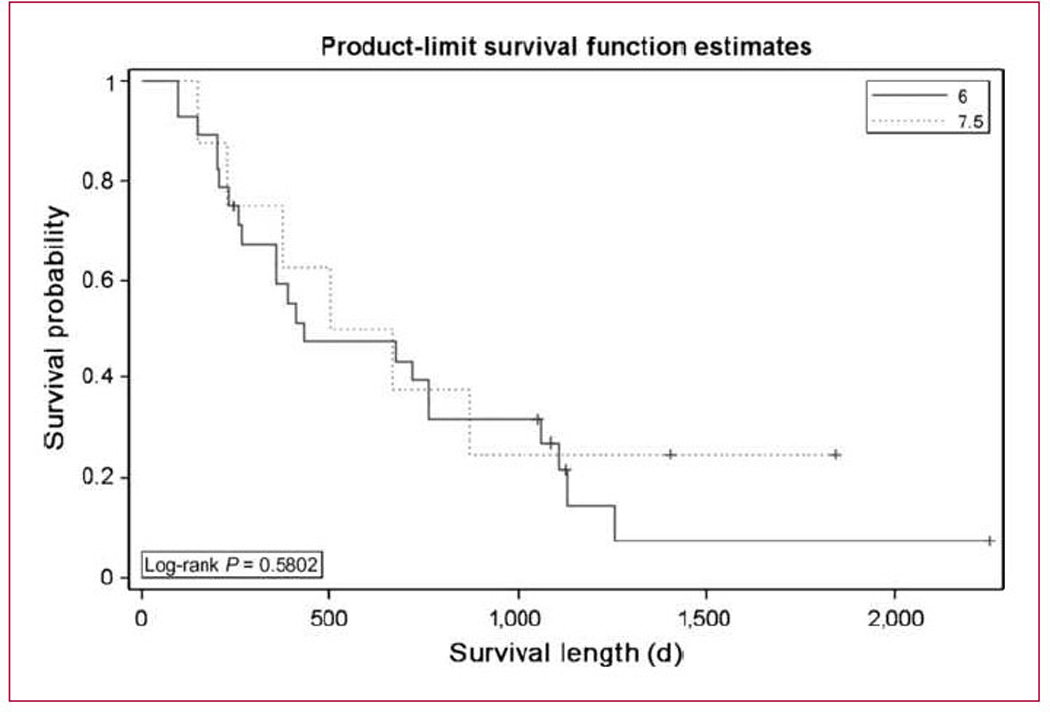
Experimental design: Patients who had chemo-naïve advanced non-small cell lung cancer were enrolled in the study. Adequate organ and pulmonary function was required: diffusing capacity for carbon monoxide/forced expiratory volume in 1 second/forced vital capacity > or =50%, resting/exercise O(2) saturation > or =90%/85%. In phase I, doxorubicin was escalated: dose level 1 (6 mg/m(2)) and level 2 (7.5 mg/m(2)). Escalation was permitted if < or =2 of 6 patients experienced pulmonary dose-limiting toxicity (grade 2 Radiation Therapy Oncology Group lung morbidity; resting O(2) saturation of <85%; decrease in diffusing capacity for carbon monoxide, forced vital capacity, or forced expiratory volume in 1 second of > or =20% from baseline or < or =30% of predicted; or grade 3 Common Terminology Criteria for Adverse Events version 3.0 pulmonary toxicity). Doses of cisplatin and docetaxel were 75 mg/m(2). Treatments and pulmonary function tests were repeated every 21 days, with up to eight cycles for responding patients.
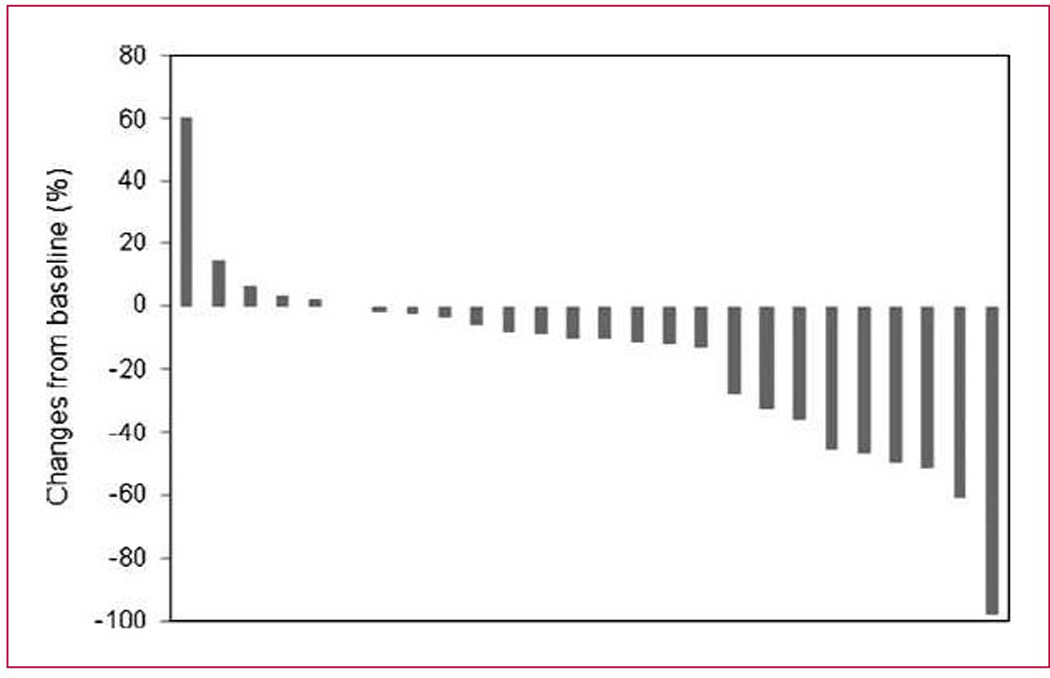
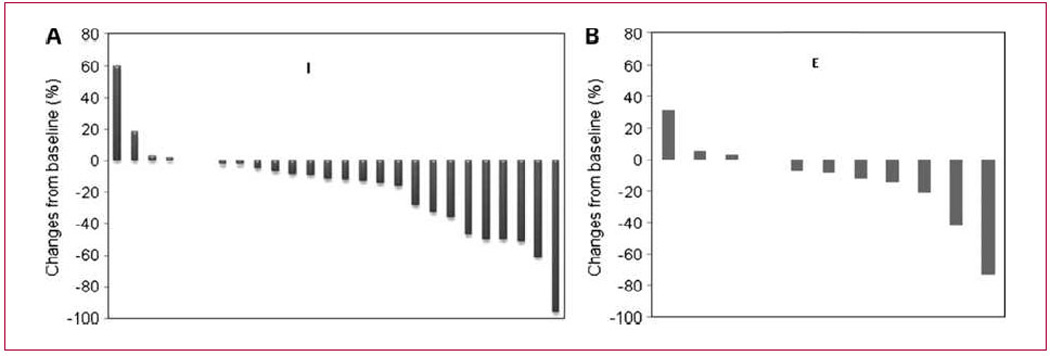
Results: Twenty-eight patients were treated at level 1 and eight patients at level 2. Doxorubicin was escalated to 7.5 mg/m(2), however, after two patients developed pulmonary dose-limiting toxicity; the remainder were treated at 6.0 mg/m(2). Twenty-four evaluable patients received at least two courses or had progressive disease following the first course at the phase II dose. Toxicity was associated with i.v. chemotherapy although one patient had delayed pulmonary toxicity responding to corticosteroids and oxygen. Seven (29%) evaluable patients responded (six partial responses and one complete response) and 13 (54%) patients had stable disease for up to eight cycles.
Conclusion: Although this combination was safe, the primary objective was not met and will not be pursued further.
Conflict of interest statement
No potential conflicts of interest were disclosed.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Schiller JH, Harrington D, Belani CP, et al. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med. 2002;346:92–98. - PubMed
-
- Sandler A, Gray R, Perry MC, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med. 2006;355:2542–2550. - PubMed
-
- Pirker R, Pereira JR, Szczesna A, et al. Cetuximab plus chemotherapy in patients with advanced non-small-cell lung cancer (FLEX): an open-label randomised phase III trial. Lancet. 2009;373:1525–1531. - PubMed
-
- Scagliotti GV, Parikh P, von Pawel J, et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer. J Clin Oncol. 2008;26:3543–3551. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
