

Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults
- PMID: 20371784
- PMCID: PMC2885954
- DOI: 10.1001/jama.2010.338
Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults
Abstract
Context: In recent decades, the fastest growth in lumbar surgery occurred in older patients with spinal stenosis. Trials indicate that for selected patients, decompressive surgery offers an advantage over nonoperative treatment, but surgeons often recommend more invasive fusion procedures. Comorbidity is common in older patients, so benefits and risks must be carefully weighed in the choice of surgical procedure.
Objective: To examine trends in use of different types of stenosis operations and the association of complications and resource use with surgical complexity.
Design, setting, and patients: Retrospective cohort analysis of Medicare claims for 2002-2007, focusing on 2007 to assess complications and resource use in US hospitals. Operations for Medicare recipients undergoing surgery for lumbar stenosis (n = 32,152 in the first 11 months of 2007) were grouped into 3 gradations of invasiveness: decompression alone, simple fusion (1 or 2 disk levels, single surgical approach), or complex fusion (more than 2 disk levels or combined anterior and posterior approach).
Main outcome measures: Rates of the 3 types of surgery, major complications, postoperative mortality, and resource use.
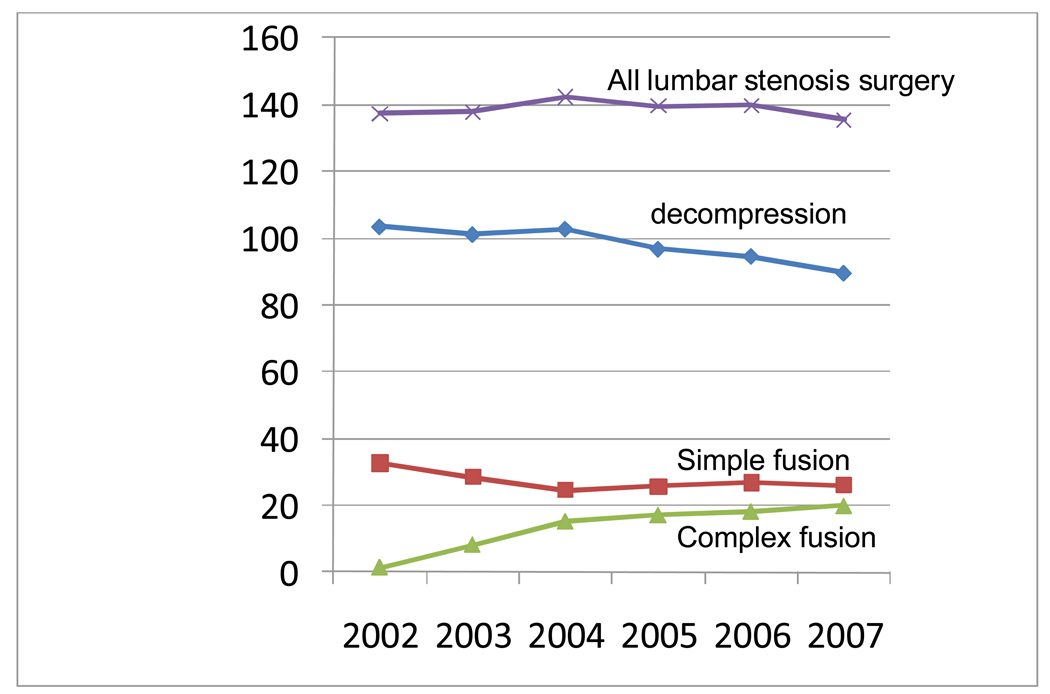
Results: Overall, surgical rates declined slightly from 2002-2007, but the rate of complex fusion procedures increased 15-fold, from 1.3 to 19.9 per 100,000 beneficiaries. Life-threatening complications increased with increasing surgical invasiveness, from 2.3% among patients having decompression alone to 5.6% among those having complex fusions. After adjustment for age, comorbidity, previous spine surgery, and other features, the odds ratio (OR) of life-threatening complications for complex fusion compared with decompression alone was 2.95 (95% confidence interval [CI], 2.50-3.49). A similar pattern was observed for rehospitalization within 30 days, which occurred for 7.8% of patients undergoing decompression and 13.0% having a complex fusion (adjusted OR, 1.94; 95% CI, 1.74-2.17). Adjusted mean hospital charges for complex fusion procedures were US $80,888 compared with US $23,724 for decompression alone.
Conclusions: Among Medicare recipients, between 2002 and 2007, the frequency of complex fusion procedures for spinal stenosis increased while the frequency of decompression surgery and simple fusions decreased. In 2007, compared with decompression, simple fusion and complex fusion were associated with increased risk of major complications, 30-day mortality, and resource use.
Figures
Comment in
-
The increasing morbidity of elective spinal stenosis surgery: is it necessary?JAMA. 2010 Apr 7;303(13):1309-10. doi: 10.1001/jama.2010.402. JAMA. 2010. PMID: 20371793 No abstract available.
-
Evidence-based recommendations for spine surgery.Spine (Phila Pa 1976). 2011 Jun 15;36(14):E897-903. doi: 10.1097/BRS.0b013e31821c06d8. Spine (Phila Pa 1976). 2011. PMID: 21642806 No abstract available.
-
Error in trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults.JAMA. 2011 Sep 14;306(10):1088. doi: 10.1001/jama.2011.1300. JAMA. 2011. PMID: 21917578 No abstract available.
-
Re: Interspinous spacers versus decompressive surgery for lumbar neurogenic intermittent claudication. Spine 2013;38:1525.Spine (Phila Pa 1976). 2013 Aug 1;38(17):1525. doi: 10.1097/BRS.0b013e3182972e08. Spine (Phila Pa 1976). 2013. PMID: 23900116 Free PMC article. No abstract available.
-
In response.Spine (Phila Pa 1976). 2013 Aug 1;38(17):1526. doi: 10.1097/BRS.0b013e31829c2e3a. Spine (Phila Pa 1976). 2013. PMID: 23900117 No abstract available.
References
-
- Irwin ZN, Hilibrand A, Gustavel M, et al. Variation in surgical decision making for degenerative spinal disorders. Part I: lumbar spine. Spine. 2005;30:2208–2213. - PubMed
-
- Katz JN, Lipson SJ, Lew RA, et al. Lumbar laminectomy alone or with instrumented or noninstrumented arthrodesis in degenerative lumbar spinal stenosis. Patient selection, costs, and surgical outcomes. Spine. 1997;22:1123–1131. - PubMed
-
- Fritzell P, Hagg O, Wessbert P, Nordwall A and the Swedish Lumbar Spine Study Group. 2001 Volvo Award winner in clinical studies: lumbar fusion versus nonsurgical treatment of chronic low back pain: a multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine. 2001;26:2521–2532. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
