

Anorectal disorders
- PMID: 20372131
- PMCID: PMC3923303
- DOI: 10.1038/ajg.2010.70
Anorectal disorders
Figures
- 1.
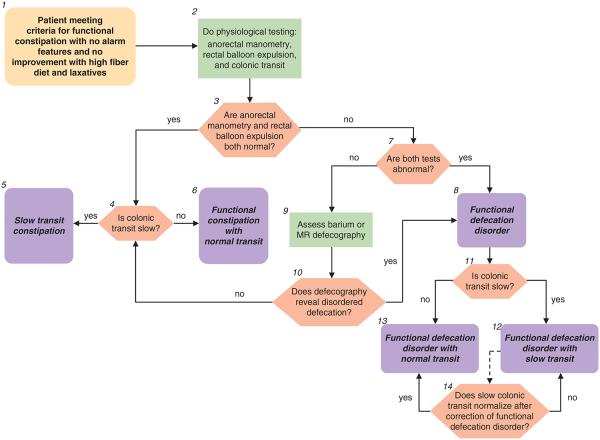
For the initial assessment of chronic constipation, and the diagnosis of functional constipation, see the preceding algorithm “chronic constipation”. Rome III diagnostic criteria for functional constipation (1) are: (i) two or more of the following: (a) straining during at least 25% of defecations, (b) lumpy or hard stools in at least 25% of defecations, (c) sensation of incomplete evacuation for at least 25% of defecations, (d) sensation of anorectal obstruction/blockage for at least 25% of defecations, (e) manual maneuvers to facilitate at least 25% of defecations (e.g., digital evacuations and support of the pelvic floor), (f) fewer than three defecations per week; and (ii) loose stools are rarely present without the use of laxatives; (iii) insufficient criteria for irritable bowel syndrome; (iv) criteria fulfilled for at least 3 months with symptom onset at least 6 months before diagnosis. The use of a stool diary incorporating the Bristol Stool Form Scale can provide more information regarding stool frequency, consistency and passage. However, in this context as well as the above information, and the presence or absence of abdominal pain linked to the disordered bowel pattern, the history should particularly establish the presence of other relevant symptoms. These include a sensation of incomplete evacuation, any sensation of anorectal obstruction and the use of manual maneuvers to aid evacuation. The absence of “alarm” features should be confirmed, namely: age >50 years, short history (<6 months), family history of colon cancer, blood in stools, and weight loss (2). Patients who fulfill the criteria for functional constipation and those who have not improved with an increase in dietary fiber and the use of simple laxatives (see “chronic constipation” algorithm), and with no alarm features, often warrant further physiological assessment. Although some physicians may, perhaps for medicolegal reasons, opt in this setting to evaluate for colon cancer with imaging or endoscopy, there is no evidence to support this practice in the absence of alarm symptoms as the prevalence of colonic neoplastic lesions at colonoscopy is comparable in patients with vs. without chronic constipation (15).
- 2.
The three key physiological investigations are anorectal manometry, the balloon expulsion test, and a colonic transit study. Anorectal manometry is carried out using water perfused or solid-state sensors or more recently by high-resolution manometry. At a minimum, anal-resting and -squeeze pressure, and the recto-anal inhibitory reflex should be assessed during manometry. Recto-anal pressure changes during straining, a maneuver which simulates defecation, should also be assessed when an evacuation disorder is suspected. Anal pressures should preferably be calculated by averaging all four quadrants to account for anal sphincter asymmetry. Variations in patient effort also need to be taken into account. Resting pressures are probably less susceptible to artifact than are squeeze pressures. Squeeze pressure should be measured by asking patients to squeeze (i.e., contract) the sphincter for at least 30 s, and to average pressure over this duration. As anal pressures are affected by age, gender, and technique, measurements ideally should be compared against normal values obtained in age- and gender-matched subjects by the same technique (16-18). The rectal balloon expulsion test, carried out by measuring the time required to expel a rectal balloon filled with 50 ml warm water or air, is a useful, relatively sensitive, and specific test for evacuation disorders (19,20). The balloon inflation volume for this test is not standardized; the balloon is either inflated by a fixed volume, typically 50–60 ml, or until patients experience the desire to defecate. When the balloon is inflated by a fixed volume (e.g., 50–60 ml), as in most laboratories, patients who have reduced rectal sensation may not perceive the desire to defecate, and therefore may be unable to expel a balloon. The performance characteristics of this test vs. defecography were evaluated by a study, in which the balloon was inflated to the volume at which patients experienced the desire to defecate. The normal value depends on the technique. At most centers, >60 s is considered as abnormal. The balloon expulsion test is a useful screening test, but does not define the mechanism of disordered defecation, nor does a normal balloon expulsion study always exclude a functional defecation disorder. Additional research is needed to standardize this test that does not always correlate with other tests of rectal emptying such as defecography and surface electromyography (EMG) recordings of the anal sphincters. Colonic transit is most readily assessed using a radio-opaque marker technique; scintigraphy and more recently, a wireless pH-pressure capsule have also been used to measure transit. Colonic transit measured by these three methods is reasonably comparable. There are several available techniques of measuring transit by radio-opaque markers. In the Hinton technique, a capsule containing 24 radio-opaque markers is given on day 1 and the remaining markers seen on a plain abdominal X-ray on day 6 are counted: <5 markers remaining in the colon is normal, >5 markers scattered throughout the colon = slow transit, and >5 markers in the recto-sigmoid region with a near normal clearance of rest of colon may suggest functional defecation disorder (21). In an alternative approach, which characterizes not only overall but also regional colonic transit, a capsule containing 24 radio-opaque markers is given on days 1, 2, and 3 and remaining markers seen on a plain abdominal X-ray on days 4 and 7 are counted (22). With this technique, a total of >68 markers remaining in the colon is normal whereas >68 markers is slow transit. *Note: Instruct radiology to use high penetration films (110 keV) to reduce radiation exposure; if <34 markers on day 4, then the second X-ray is not required. Have patient avoid laxatives and keep diary of bowel movements for 1 week before, and during, the test to correlate with transit. Colonic transit can also be measured by a wireless motility-pH capsule. In constipated patients, the correlation between colonic transit measured by radio-opaque markers (on day 5) and the capsule is reasonable (correlation coefficient of approximately 0.7) (23). The capsule can also measure colonic motor activity (24). Scintigraphy entails delivering an isotope (generally 99 mTc or 111 In) into the colon by a delayed-release capsule that has a pH-sensitive polymer (methacrylate), which dissolves in the alkaline pH of the distal ileum, releasing the radioisotope within the ascending colon. Then, gamma camera scans taken 4, 24, and, if necessary, 48 h after the isotope was ingested show the colonic distribution of isotope (25). Advantages of scintigraphy are that colonic transit can be assessed in 48 h as opposed to 5–7 days for radio-opaque markers. Also, gastric, small intestinal, and colonic transit can be simultaneously assessed by scintigraphy.
- 3.
At anal manometry, the patterns of anal sphincter and rectal pressure changes during attempted defecation are the most relevant parameters in this context. A normal pattern is characterized by increased intrarectal pressure associated with relaxation of the anal sphincter. Abnormal patterns are characterized by lower rectal than anal pressures during expulsion effort, resulting from the inability to generate an adequate propulsive or “pushing” intra-rectal pressure, and/or impaired relaxation or paradoxical contraction of the anal sphincter. However, as a proportion of asymptomatic subjects may have an abnormal pattern, it is necessary to interpret this test in the context of clinical features and other test results.
- 4–6.
If both anorectal manometry and balloon expulsion are normal, the results of colonic transit testing enable characterization of the disorder as functional constipation with normal or slow transit. The normal values for the radio-opaque marker tests are given above. Some patients with slow and even normal transit constipation have colonic motor dysfunction, perhaps severe enough to be characterized by colonic inertia. On the other hand, slow transit constipation may be associated with normal colonic motor functions, as assessed by intraluminal methods (i.e., a barostat or manometry), or with defecatory disorders (26). Although the diagnostic criteria for colonic inertia are not established, this term refers to reduced contractile responses, measured by manometry and/or a barostat, to physiological (i.e., a meal), and pharmacological stimuli (e.g., bisacodyl and neostigmine) stimuli. Colonic manometry and barostat testing is available at selected centers. The clinical utility of distinguishing between colonic motor dysfunction and inertia is unknown. A hypaque enema should be considered if plain abdominal X-rays suggest megacolon.
- 7,8.
Based on results of recent studies, if both manometry and the rectal balloon expulsion test are abnormal, this is sufficient to diagnose a functional defecation disorder (20) In this circumstance imaging (e.g., barium or MR defecography) is not generally required but should be considered if it is necessary to exclude a structural abnormality e.g., enteroceles, intussusception, or clinically significant rectoceles. Although clinical features and digital rectal examination can identify a rectocele, imaging can assess its size and emptying during evacuation. The Rome III diagnostic criteria for functional defecation disorders are: (i) the patient must satisfy diagnostic criteria for functional constipation; (ii) during repeated attempts to defecate, must have at least two of the following: (a) evidence of impaired evacuation, based on balloon expulsion test or imaging, (b) inappropriate contraction of the pelvic floor muscles (i.e., anal sphincter or puborectalis) or <20% relaxation of basal resting sphincter pressure by manometry, imaging or EMG, and (c) inadequate propulsive forces assessed by manometry or imaging; (3) criteria fulfilled for the last 3 months with symptom onset at least 6 months before diagnosis. Inappropriate anal contraction is also referred to as dyssynergic defecation.
- 9.
If only one of the anorectal manometry and balloon expulsion is abnormal, further testing—barium or magnetic resonance defecography may be used to confirm or exclude the diagnosis. Defecography can detect structural abnormalities (rectocele, enterocele, rectal prolapse, and intussusception) and assess functional parameters (anorectal angle at rest and during straining, perineal descent, anal diameter, indentation of the puborectalis, and amount of rectal and rectocele emptying). Small bowel opacification is required to identify enterocoeles by barium defecography. The diagnostic value of defecography has been questioned primarily because normal ranges for quantified measures are inadequately defined and because some parameters such as the anorectal angle cannot be measured reliably because of variations in rectal contour. Moreover, similar to anorectal manometry, a small fraction of asymptomatic healthy people have features of disordered defecation during proctography. Thus, there is no true gold standard diagnostic test for defecation disorders. Nonetheless, an integrated consideration of tests (i.e., manometry, rectal balloon expulsion, and defecography) together with the clinical features generally suffices to confirm or exclude defecation disorders. Magnetic resonance defecography provides an alternative approach to image anorectal motion and rectal evacuation in real time without radiation exposure. In a controlled study, magnetic resonance defecography identified disturbances of evacuation and/or squeeze in 94% of patients with suspected defecation disorders (26). Whether magnetic resonance defecography will add a new dimension to the morphological and functional assessment of these patients in clinical practice merits appraisal.
- 10.
If defecography reveals features of disordered defecation, a diagnosis of a functional defecation disorder can be made. Defecographic features of disordered defecation include less than complete anal opening, impaired puborectalis relaxation or paradoxical puborectalis contraction, reduced or increased perineal descent, and a large (>4 cm) rectocoele, particularly if emptying is incomplete. If defecography is not abnormal, then the patient does not fulfill criteria for the diagnosis of a functional defecation disorder; further diagnosis then depends on the presence or absence of colonic transit delay (see above #4–6).
- 11–13.
The presence of a functional defecation disorder does not exclude the diagnosis of slow colonic transit. Thus, depending on the results of the colonic transit study, the patient can be characterized as suffering from a functional defecation disorder with normal or slow colonic transit.
- 14.
As well as coexisting with it; however, slow colonic transit may result from a defecation disorder. If it is felt appropriate to distinguish between the two possibilities, the colonic transit evaluation may be repeated after correction of the defecation disorder. If transit normalizes, the presumption is that the delay was secondary to the defecation disorder; if not, the delayed colonic transit is presumed to be a comorbid condition, which may require therapy if there is no clinical improvement with the treatment of functional defecation disorder.
- 1.
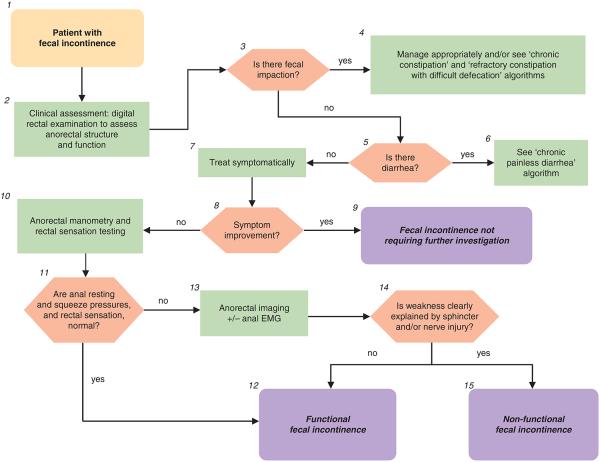
Fecal incontinence (FI) is defined as uncontrolled passage of fecal material recurring for at least 3 months in people aged 4 or more years. Leakage of flatus alone should not be characterized as FI. In this context, the FI is assumed to not be associated with known systemic or organic disorders (e.g., dementia, multiple sclerosis, and Crohn’s disease) (27,28).
- 2.
The history should determine the duration of symptoms, type of FI, and associated bowel habits; urinary and neurological symptoms should be evaluated (27). Consider possible undiagnosed systemic or organic disorders that can cause FI. Although a spinal cord lesion can cause FI, typically, patients with a spinal cord lesion and FI will have other neurological symptoms and signs of the underlying lesion. Severity is established by consideration of four variables, i.e., frequency, type (i.e., liquid, solid stool, or both), amount (small, moderate, or large) of leakage, and presence/absence of urgency. The physical examination should particularly evaluate the presence of any alarm signs e.g., abdominal mass, evidence of anemia. Where indicated, a neurological examination should be carried out. A careful digital rectal examination is critical to understanding the etiology and for guiding management of FI. This should assess for stool impaction, anal resting tone (patients with markedly reduced tone may have a gaping sphincter), contraction of the external sphincter and puborectalis to voluntary command, and/or dyssynergia during simulated evacuation. In this patient, anal-squeeze response was reduced but the puborectalis lift was preserved, consistent with sphincter but not puborectalis weakness. Dyssynergia refers to impaired relaxation and/or paradoxical contraction of the anal sphincter and/or puborectalis muscle and/or reduced perineal descent during simulated evacuation. To evaluate the integrity of the sacral lower motor neuron reflex arc, perianal pinprick sensation, and the anal wink reflex should also be assessed.
- 3.
The presence of fecal impaction at digital rectal examination suggests fecal retention and “overflow” FI. An abdominal X-ray should be considered to identify colonic fecal retention if appropriate.
- 4.
If fecal impaction is present, see “chronic constipation” and “refractory constipation” algorithms. If FI persists after appropriate treatment of the fecal impaction, consider further evaluation for FI as described below.
- 5,6.
Patients with FI and moderate to severe diarrhea should be investigated appropriately as detailed in “chronic painless diarrhea” algorithm. If FI persists after appropriate treatment of the diarrhea, consider further evaluation for FI as continued below.
- 6.
Patients with mild symptoms and/or symptoms that are not bothersome will often benefit from symptomatic management of the FI and any associated bowel disturbances, often on an as-needed basis (29). Such management may include a trial of loperamide and/or bulking agents, advice regarding the role of scheduled evacuation, and if necessary, the use of perineal protective devices. Patients with passive incontinence for a small amount of stool may benefit from a perianal cotton plug to absorb moisture and also perhaps to help with uncontrolled passage of gas.
- 8,9.
If symptoms improve and there are no features to suggest an organic disorder (e.g., neurological symptoms/signs suggestive of a spinal cord lesion), further testing may not be necessary—see comment number 10). A diagnosis of FI, without qualifying whether organic or functional as defined below, may be made.
- 10.
If symptoms do not improve, further diagnostic testing, in particular anorectal manometry, should be considered. The extent of such testing is tailored to the patient’s age, probable etiological factors, symptom severity, effect on quality of life, response to conservative medical management, and availability of tests. Although widely available, these tests should preferably be carried out by laboratories with requisite expertise.
- 11.
The key features at anorectal manometry are anal sphincter-resting and -squeeze pressures. As anal sphincter pressures decline with age and are lower in women, the age and gender should be taken into consideration when interpreting anal pressures (30-32). The anal cough reflex is useful, in a qualitative sense, for evaluating the integrity of the lower motor neuron innervation of the external anal sphincter. It is useful to assess rectal sensation, which may be normal, increased, or decreased in FI, as these disturbances can be modulated by biofeedback therapy (27).
- 12.
If these pressures are normal, a diagnosis of functional FI can be made. In addition, it is increasingly recognized that anorectal assessments may reveal disturbances of anorectal structure and/or function in patients who were hitherto considered to have an “idiopathic” or “functional” disorder. The causal relationship between structural abnormalities and anorectal function or bowel symptoms may be unclear, because such abnormalities are often observed in asymptomatic subjects (30,32). For example, up to one-third of all women have anal sphincter defects after vaginal delivery (27). As sophisticated tests (e.g., anal electromyography (EMG)) for elucidating the mechanisms of anal weakness are not widely available, the diagnosis of functional FI can also be entertained in patients, as exemplified in this case, with potentially abnormal innervation and either minor or no structural abnormalities. The Rome III diagnostic criteria for functional FI are (i) recurrent uncontrolled passage of fecal material in an individual with a developmental age of at least 4 years and one or more of the following: abnormal functioning of normally innervated and structurally intact muscles; minor abnormalities of sphincter structure and/or innervation; normal or disordered bowel habits (i.e., fecal retention or diarrhea); or psychological causes and (ii) exclusion of all of the following: abnormal innervation caused by lesion(s) within the brain (e.g., dementia), spinal cord or sacral nerve roots, or mixed lesions (e.g., multiple sclerosis), or as part of a generalized peripheral or autonomic neuropathy (e.g., diabetes); anal sphincter abnormalities associated with a multisystem disease (e.g., scleroderma); or structural or neurogenic abnormalities believed to be the major or primary cause of FI (iii) criteria fulfilled for the last 3 months.
- 13.
If the sphincter pressures are abnormal, imaging of the anal sphincter should be considered. Endoanal ultrasound and magnetic resonance imaging are probably equivalent for imaging the internal sphincter (8,31,32). Magnetic resonance imaging is better for visualizing external sphincter and puborectalis atrophy and also visualizes pelvic floor motion in real-time without radiation exposure. Anal sphincter EMG should be considered in patients with clinically suspected neurogenic sphincter weakness, particularly if there are features suggestive of proximal (i.e., sacral root) involvement (8).
- 14.
Diagnostic tests (e.g., endoanal ultrasound) may reveal disturbances of anorectal structure and/or function in patients with FI. The extent to which structural disturbances (e.g., anal sphincter defects, excessive perineal descent) can explain symptoms is often unclear (28). Therefore, the presence of structural abnormalities is not necessarily inconsistent with the diagnosis of functional FI. Many patients with anal sphincter weakness may have a pudendal neuropathy. However, it can be difficult to document a pudendal neuropathy because anal sphincter EMG requires considerable expertise and is not widely available (30,32). Therefore, patients with a pudendal neuropathy not attributable to a generalized disease process have not been excluded from the category of functional FI. A controlled study suggests that patients with FI who do not benefit from dietary modification and measures to regulate bowel habits may benefit from pelvic floor retraining (33).
- 15.
The following conditions would be considered as secondary or non-functional FI: abnormal innervation caused by lesion(s) within the spinal cord or sacral nerve roots or part of a generalized peripheral or autonomic neuropathy, anal sphincter abnormalities associated with a multi-system disease (e.g. scleroderma), and structural abnormalities believed to be the major or primary cause of the FI (28).
- 1.
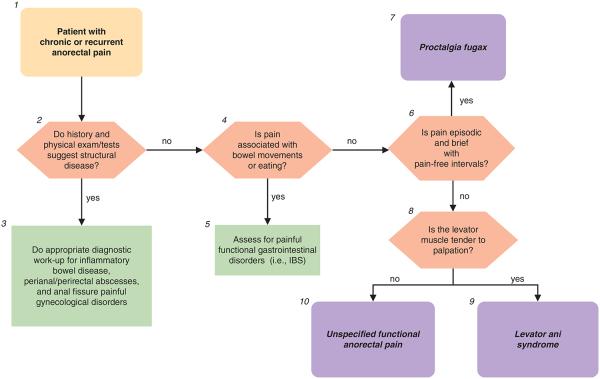
Pain present for at least 6 months is required for the diagnosis of functional anorectal pain syndrome. Patients with chronic anorectal pain have chronic or recurrent anorectal pain; if recurrent, pain lasts for 20 min or longer during episodes. In contrast, patients with proctalgia fugax have brief episodes of pain lasting seconds to minutes with no pain between episodes (28).
- 2–3.
The history and physical exam should identify alarm and other features suggesting structural disease such as severe throbbing pain, sentinel piles, fistulous opening, and anal tenderness during digital examination, or while gently parting the posterior anus, anal strictures, or induration (34). Relevant organic causes of pain including inflammatory bowel disease, peri-anal abscesses, anal fissure, and painful gynecological conditions should be considered and identified by tests. If pain is associated with and worsened by menses, conditions that might include endometriosis, dysfunctional uterine bleeding, or other gynecological pathology should be evaluated by pelvic examination, pelvic ultrasound, and/or referral to a gynecologist. Minimal diagnostic work-up (in the absence of alarm signs) includes: CBC, ESR, biochemistry panel, flexible sigmoidoscopy, and perianal imaging with ultrasound or MRI. If there is a high index of suspicion for anal fissures, anoscopy should be considered.
- 4–5.
Pain associated with bowel movements, menses or eating, excludes the diagnosis of functional anorectal pain. If pain is associated with bowel movements and leads to frequent, looser stools, or infrequent harder stools with relief upon defecation (any combination of two), then a diagnosis of IBS should be considered. See “recurrent abdominal pain and disordered bowel habit” algorithm.
- 6.
An important feature of the history is whether the pain is episodic, with pain-free intervals, or not. In chronic proctalgia, pain is generally prolonged (i.e., lasts for hours), is constant or frequent, and is characteristically dull. In proctalgia fugax, the pain is brief (i.e., lasting seconds to minutes), occurs infrequently (i.e., once a month or less often), and is relatively sharp. Observation of symptom-reporting behaviors is also important. These include verbal and non-verbal expression of pain, urgent reporting of intense symptoms, minimization of a role for psychosocial contributors, requesting diagnostic studies or even exploratory surgery, focusing on complete relief of symptoms, seeking health care frequently, taking limited personal responsibility for self-management, and making requests for narcotic analgesics.
- 7.
Rome III diagnostic criteria for proctalgia fugax include all of the following: (i) recurrent episodes of pain localized to the anus or lower rectum; (ii) episodes last from seconds to minutes; and (iii) there is no anorectal pain between episodes.
- 8.
Rome III diagnostic criteria for chronic proctalgia include all of the following: (i) chronic or recurrent rectal pain or aching; (ii) episodes last 20 min or longer; (iii) exclusion of other causes of rectal pain such as ischemia, inflammatory bowel disease, cryptitis, intramuscular abscess, anal fissure, hemorrhoids, prostatitis, and coccygodynia; (iv) criteria fulfilled for last 3 months with symptom onset at least 6 months before diagnosis. In chronic proctalgia, levator ani tenderness differentiates levator ani syndrome from unspecified functional anorectal pain. Coccygodynia is characterized by pain and point tenderness of the coccyx (9). Most patients with rectal, anal, and sacral discomfort have levator rather than coccygeal tenderness (10).
- 9.
Rome III diagnostic criteria for levator ani syndrome include symptom criteria for chronic proctalgia and tenderness during posterior traction on the puborectalis muscle.
- 10.
Rome III diagnostic criteria for unspecified functional anorectal pain include symptom criteria for chronic proctalgia, but no tenderness during posterior traction on the puborectalis muscle. In a patient with levator ani syndrome, anorectal manometry and rectal balloon expulsion testing should be considered. A recent study suggests that approximately 85% patients with levator ani syndrome had impaired anal relaxation during straining and approximately 85% had abnormal rectal balloon expulsion. It is unclear if dyssynergia is a cause of or secondary to pain. However, dyssynergia may guide management as discussed below. Treatment options to present to the patient can then be formulated. A randomized control trial showed that inhalation of salbutamol (a beta adrenergic agonist) was more effective than placebo for shortening the duration of episodes of proctalgia for patients in whom episodes lasted 20 min or longer (35). In a controlled study of 157 patients with levator ani syndrome, adequate relief of pain was more likely after biofeedback therapy for a concomitant evacuation disorder (87%) than electrogalvanic stimulation (EGS) (45%) or rectal digital massage (22%) (36). Biofeedback and EGS also improved pelvic floor relaxation in levator ani syndrome. In contrast, none of these measures benefited patients with functional anorectal pain. Although features of disordered defecation did not augment the utility of levator tenderness for predicting a response to biofeedback therapy, it is useful to assess defecatory functions because (i) the presence of dyssynergia before training and improvement thereof after training was very highly correlated with the success of biofeedback (and also EGS), and (ii) the biofeedback protocol is more logical to patients and providers in the presence of dyssynergia. Other treatment options include TC A or SSRI therapy or non-pharmacological therapy such as cognitive behavioral therapy (CBT), hypnotherapy, or dynamic or interpersonal psychotherapy.
Similar articles
-
Pediatric anorectal disorders.Gastroenterol Clin North Am. 2008 Sep;37(3):709-30, x. doi: 10.1016/j.gtc.2008.07.002. Gastroenterol Clin North Am. 2008. PMID: 18794005 Review.
-
[Anorectal functional tests--essence and value].Khirurgiia (Sofiia). 2003;59(1-2):46-50. Khirurgiia (Sofiia). 2003. PMID: 15587745 Bulgarian.
-
[Value and limits of clinical examination to functional anorectal disorders (except for chronic anorectal pain)].Gastroenterol Clin Biol. 2003 May;27(5 Suppl):B87-98. Gastroenterol Clin Biol. 2003. PMID: 12843942 Review. French. No abstract available.
-
Functional disorders of the anus and rectum.Gut. 1999 Sep;45 Suppl 2(Suppl 2):II55-9. doi: 10.1136/gut.45.2008.ii55. Gut. 1999. PMID: 10457046 Free PMC article. Review.
-
Common anorectal disorders: diagnosis and treatment.Curr Gastroenterol Rep. 2009 Oct;11(5):413-9. doi: 10.1007/s11894-009-0062-y. Curr Gastroenterol Rep. 2009. PMID: 19765370
Cited by
-
Current Incidence and Risk Factors of Fecal Incontinence After Acute Stroke Affecting Functionally Independent People.Front Neurol. 2021 Nov 1;12:755432. doi: 10.3389/fneur.2021.755432. eCollection 2021. Front Neurol. 2021. PMID: 34790163 Free PMC article.
-
An update on anorectal disorders for gastroenterologists.Gastroenterology. 2014 Jan;146(1):37-45.e2. doi: 10.1053/j.gastro.2013.10.062. Epub 2013 Nov 6. Gastroenterology. 2014. PMID: 24211860 Free PMC article. Review.
-
Biofeedback for treatment of chronic idiopathic constipation in adults.Cochrane Database Syst Rev. 2014 Mar 26;2014(3):CD008486. doi: 10.1002/14651858.CD008486.pub2. Cochrane Database Syst Rev. 2014. PMID: 24668156 Free PMC article.
-
Pathoetiology of Levator Ani Syndrome and Its Treatment With Translumbosacral Neuromodulation Therapy.Am J Gastroenterol. 2023 Dec 1;118(12):2242-2246. doi: 10.14309/ajg.0000000000002394. Epub 2023 Jul 7. Am J Gastroenterol. 2023. PMID: 37410923 Free PMC article.
-
A randomised controlled study of the effect of cholinesterase inhibition on colon function in patients with diabetes mellitus and constipation.Gut. 2013 May;62(5):708-15. doi: 10.1136/gutjnl-2012-302483. Epub 2012 Jun 7. Gut. 2013. PMID: 22677718 Free PMC article. Clinical Trial.
References
-
- Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scand J Gastroenterol. 1997;32:920–4. - PubMed
-
- Mertz H, Naliboff B, Mayer EA. Symptoms and physiology in severe chronic constipation. Am J Gastroenterol. 1999;94:131–8. - PubMed
-
- Andrews CN, Bharucha AE. The etiology, assessment, and treatment of fecal incontinence. Nat Clin Pract Gastroenterol Hepatol. 2005;2:516–25. - PubMed
-
- Leigh RJ, Turnberg LA. Faecal incontinence: the unvoiced symptom. Lancet. 1982;1:1349–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
