

Goal-directed coagulation management of major trauma patients using thromboelastometry (ROTEM)-guided administration of fibrinogen concentrate and prothrombin complex concentrate
- PMID: 20374650
- PMCID: PMC2887173
- DOI: 10.1186/cc8948
Goal-directed coagulation management of major trauma patients using thromboelastometry (ROTEM)-guided administration of fibrinogen concentrate and prothrombin complex concentrate
Abstract
Introduction: The appropriate strategy for trauma-induced coagulopathy management is under debate. We report the treatment of major trauma using mainly coagulation factor concentrates.
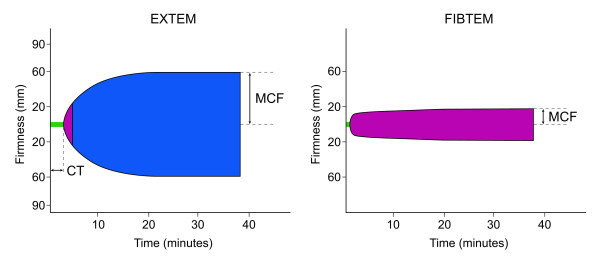
Methods: This retrospective analysis included trauma patients who received >or= 5 units of red blood cell concentrate within 24 hours. Coagulation management was guided by thromboelastometry (ROTEM). Fibrinogen concentrate was given as first-line haemostatic therapy when maximum clot firmness (MCF) measured by FibTEM (fibrin-based test) was <10 mm. Prothrombin complex concentrate (PCC) was given in case of recent coumarin intake or clotting time measured by extrinsic activation test (EXTEM) >1.5 times normal. Lack of improvement in EXTEM MCF after fibrinogen concentrate administration was an indication for platelet concentrate. The observed mortality was compared with the mortality predicted by the trauma injury severity score (TRISS) and by the revised injury severity classification (RISC) score.
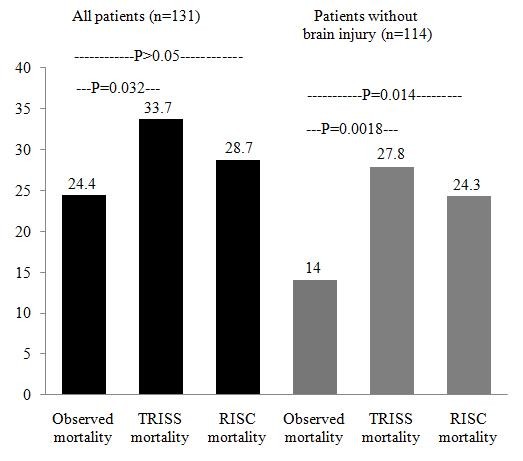
Results: Of 131 patients included, 128 received fibrinogen concentrate as first-line therapy, 98 additionally received PCC, while 3 patients with recent coumarin intake received only PCC. Twelve patients received FFP and 29 received platelet concentrate. The observed mortality was 24.4%, lower than the TRISS mortality of 33.7% (P = 0.032) and the RISC mortality of 28.7% (P > 0.05). After excluding 17 patients with traumatic brain injury, the difference in mortality was 14% observed versus 27.8% predicted by TRISS (P = 0.0018) and 24.3% predicted by RISC (P = 0.014).
Conclusions: ROTEM-guided haemostatic therapy, with fibrinogen concentrate as first-line haemostatic therapy and additional PCC, was goal-directed and fast. A favourable survival rate was observed. Prospective, randomized trials to investigate this therapeutic alternative further appear warranted.
Figures
Comment in
-
Traditional transfusion practices are changing.Crit Care. 2010;14(3):162. doi: 10.1186/cc9009. Epub 2010 Jun 1. Crit Care. 2010. PMID: 20550726 Free PMC article.
References
-
- Spahn DR, Cerny V, Coats TJ, Duranteau J, Fernandez-Mondejar E, Gordini G, Stahel PF, Hunt BJ, Komadina R, Neugebauer E, Ozier Y, Riddez L, Schultz A, Vincent JL, Rossaint R. Management of bleeding following major trauma: a European guideline. Crit Care. 2007;11:R17. doi: 10.1186/cc5686. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
