

Mutations in fibrillin-1 cause congenital scleroderma: stiff skin syndrome
- PMID: 20375004
- PMCID: PMC2953713
- DOI: 10.1126/scitranslmed.3000488
Mutations in fibrillin-1 cause congenital scleroderma: stiff skin syndrome
Abstract
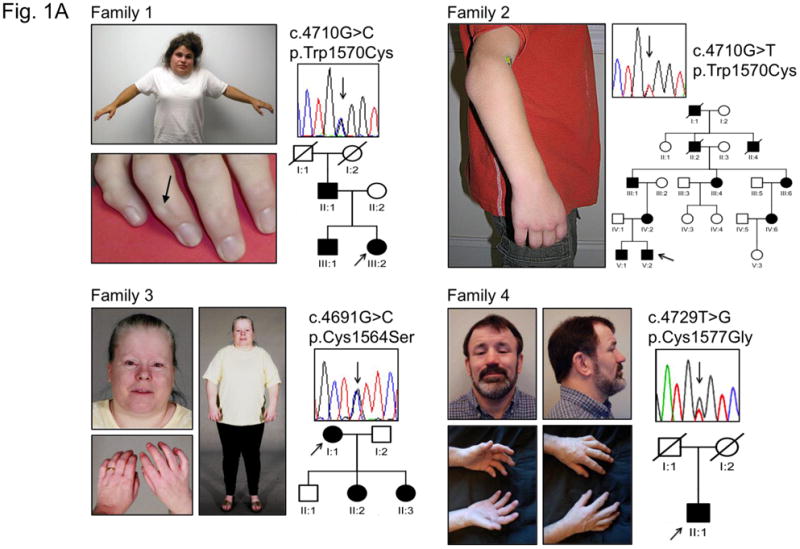
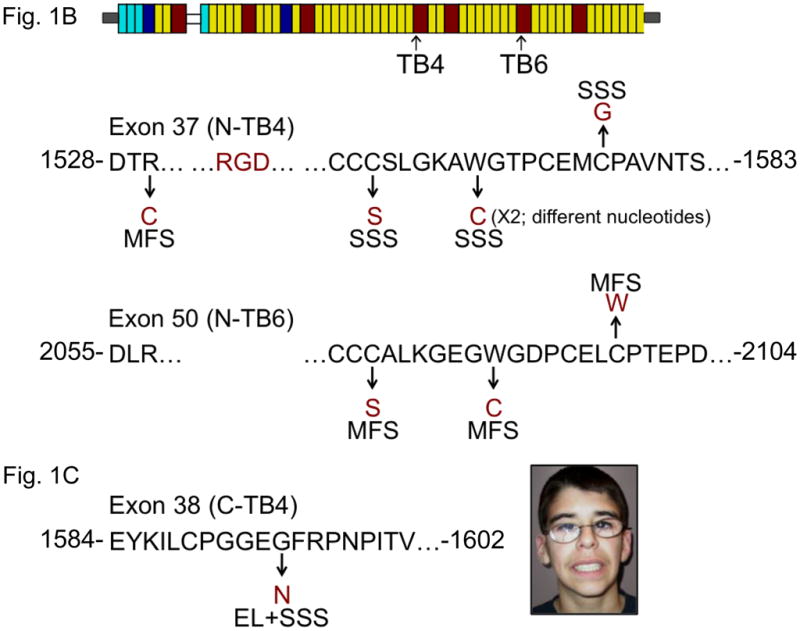
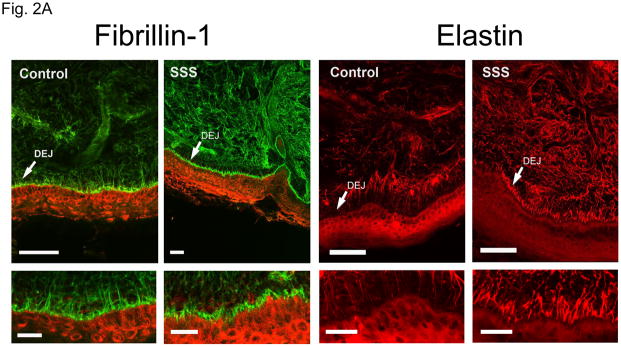
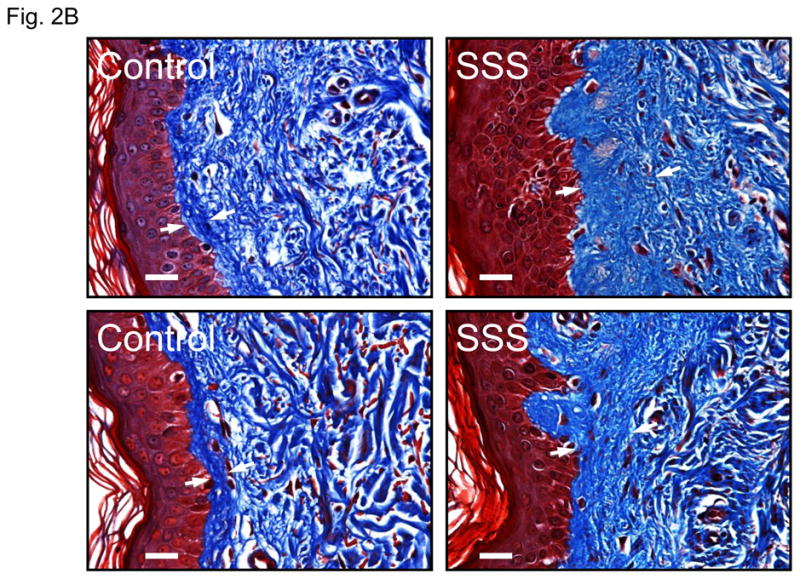
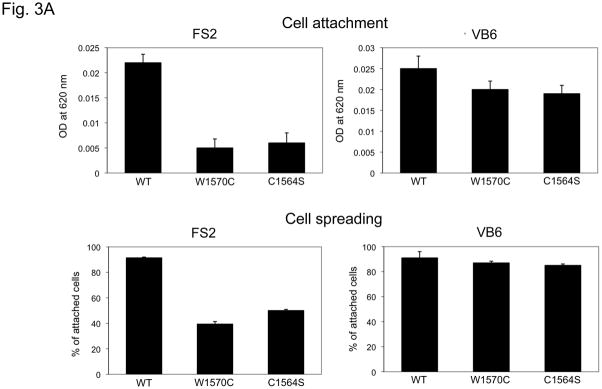
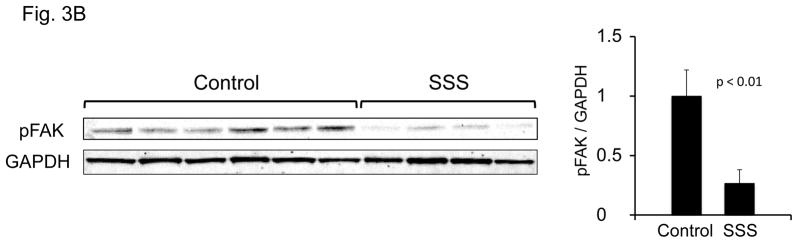
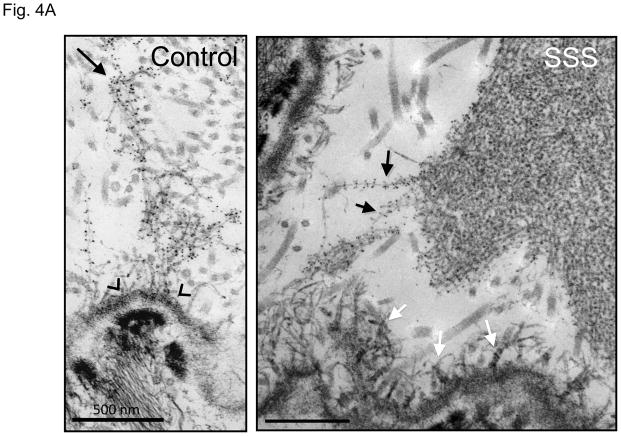
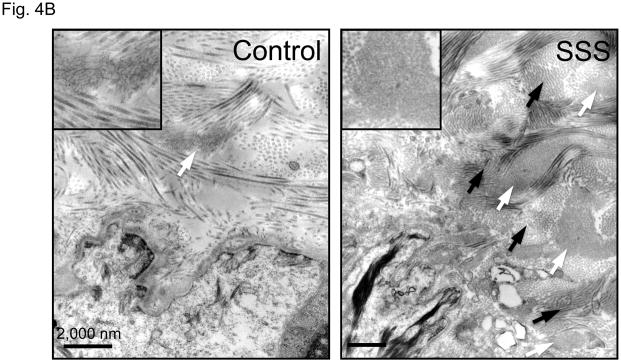
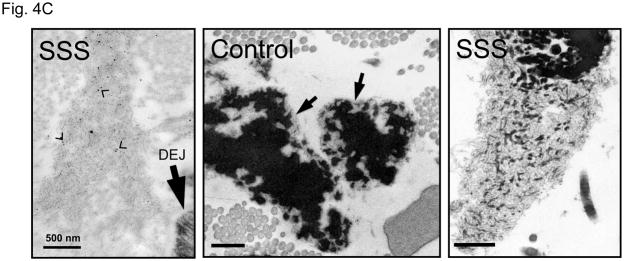
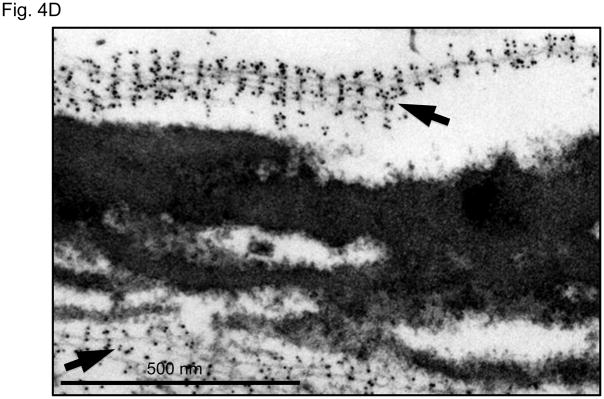
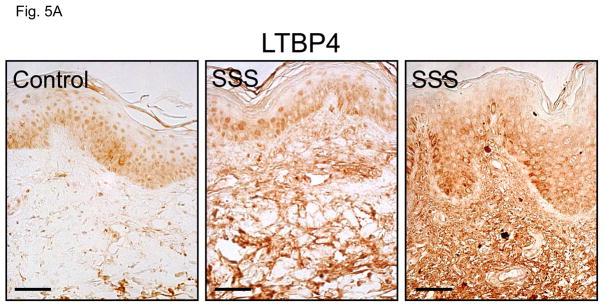
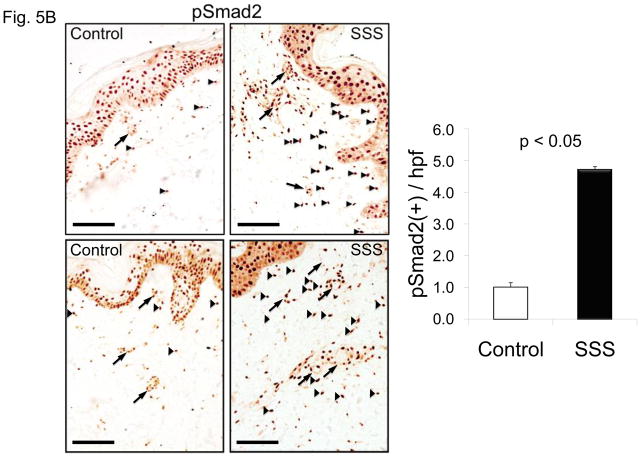
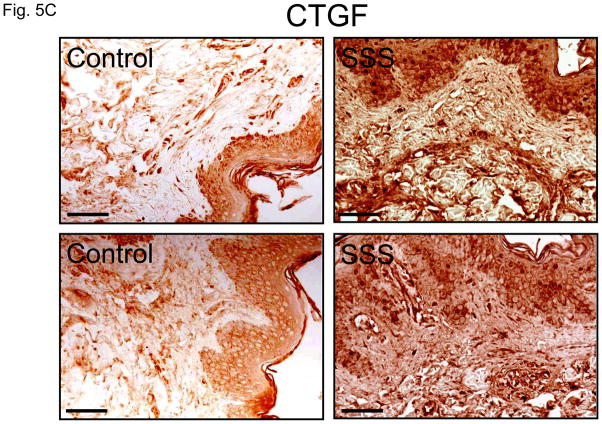
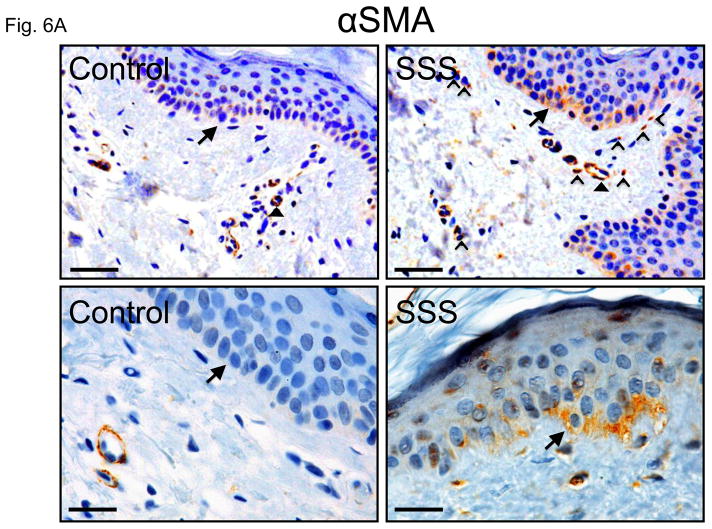
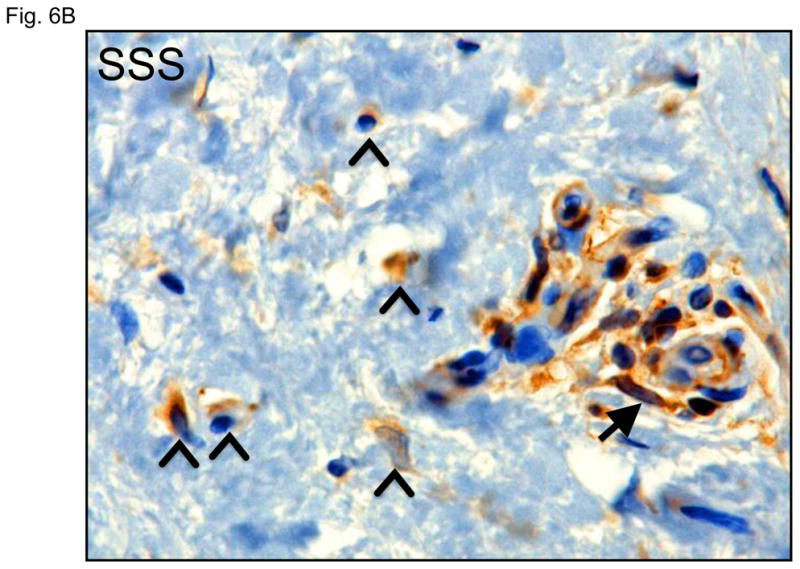
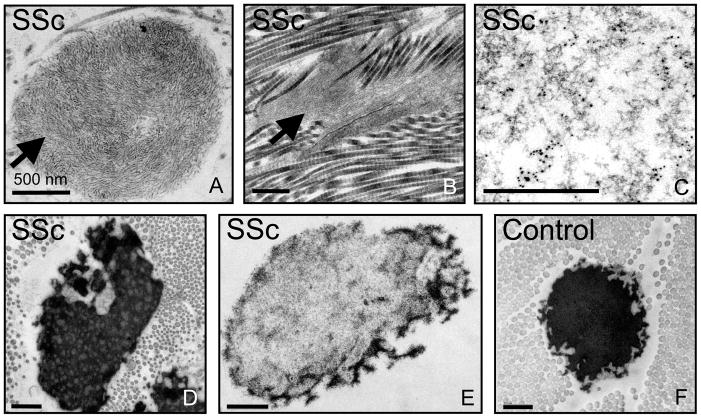
The predisposition for scleroderma, defined as fibrosis and hardening of the skin, is poorly understood. We report that stiff skin syndrome (SSS), an autosomal dominant congenital form of scleroderma, is caused by mutations in the sole Arg-Gly-Asp sequence-encoding domain of fibrillin-1 that mediates integrin binding. Ordered polymers of fibrillin-1 (termed microfibrils) initiate elastic fiber assembly and bind to and regulate the activation of the profibrotic cytokine transforming growth factor-beta (TGFbeta). Altered cell-matrix interactions in SSS accompany excessive microfibrillar deposition, impaired elastogenesis, and increased TGFbeta concentration and signaling in the dermis. The observation of similar findings in systemic sclerosis, a more common acquired form of scleroderma, suggests broad pathogenic relevance.
Figures
Comment in
-
Stiff and tight skin: a rear window into fibrosis without inflammation.Sci Transl Med. 2010 Mar 17;2(23):23ps13. doi: 10.1126/scitranslmed.3000949. Sci Transl Med. 2010. PMID: 20375002
References
-
- Wigley FM. Vascular disease in scleroderma. Clin Rev Allergy Immunol. 2009;36:150–175. - PubMed
-
- Esterly NB, McKusick VA. Stiff skin syndrome. Pediatrics. 1971;47:360–369. - PubMed
-
- Amoric JC, Stalder JF, David A, Bureau B, Pierard GE, Litoux P. Dysmorphism in Stiff Skin syndrome. Ann Dermatol Venereol. 1991;118:802–804. - PubMed
-
- Bodemer C, Habib K, Teillac D, Munich A, de Prost Y. A new case of Stiff Skin syndrome. Ann Dermatol Venereol. 1991;118:805–806. - PubMed
-
- Bundy SE, Lie K. Stiff skin syndrome. Birth Defects Orig Artic Ser. 1975;11:360–361. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
