

The ABCs of rhinoviruses, wheezing, and asthma
- PMID: 20375160
- PMCID: PMC2897627
- DOI: 10.1128/JVI.02290-09
The ABCs of rhinoviruses, wheezing, and asthma
Abstract
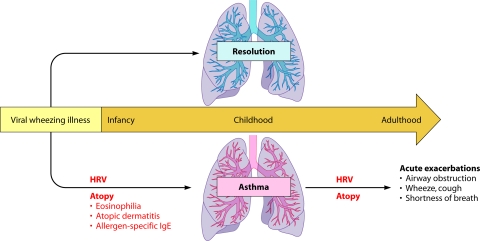
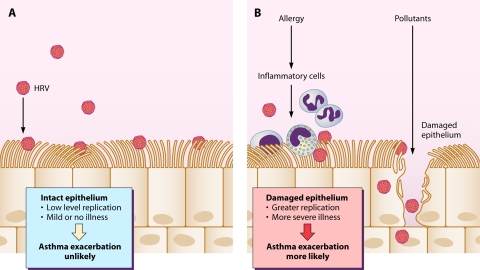
Human rhinoviruses (HRVs) were discovered as common cold pathogens over 50 years ago. Recent advances in molecular viral diagnostics have led to an appreciation of their role in more-significant respiratory illnesses, including bronchiolitis in infancy, childhood pneumonia, and acute exacerbations of chronic respiratory diseases such as asthma, chronic obstructive lung disease, and cystic fibrosis. Until a few years ago, only two groups of HRVs (A and B) had been recognized. However, full and partial sequencing of HRVs led to the discovery of a third species of HRV (HRV-C) that has distinct structural and biologic features. Risk factors and pathogenic mechanisms for more-severe HRV infections are being defined, and yet fundamental questions persist about mechanisms relating this common pathogen to allergic diseases and asthma. The close relationship between HRV infections and asthma suggests that antiviral treatments could have a major impact on the morbidity associated with this chronic respiratory disease.
Figures
References
-
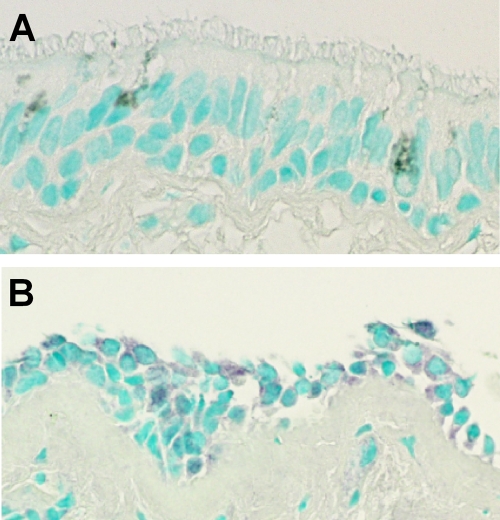
- Arruda, E., T. R. Boyle, B. Winther, D. C. Pevear, J. M. Gwaltney, and F. G. Hayden. 1995. Localization of human rhinovirus replication in the upper respiratory tract by in situ hybridization. J. Infect. Dis. 171:1329-1333. - PubMed
-
- Atmar, R. L., E. Guy, K. K. Guntupalli, J. L. Zimmerman, V. D. Bandi, B. D. Baxter, and S. B. Greenberg. 1998. Respiratory tract viral infections in inner-city asthmatic adults. Arch. Intern. Med. 158:2453-2459. - PubMed
-
- Bartlett, N. W., R. P. Walton, M. R. Edwards, J. Aniscenko, G. Caramori, J. Zhu, N. Glanville, K. J. Choy, P. Jourdan, J. Burnet, T. J. Tuthill, M. S. Pedrick, M. J. Hurle, C. Plumpton, N. A. Sharp, J. N. Bussell, D. M. Swallow, J. Schwarze, B. Guy, J. W. Almond, P. K. Jeffery, C. M. Lloyd, A. Papi, R. A. Killington, D. J. Rowlands, E. D. Blair, N. J. Clarke, and S. L. Johnston. 2008. Mouse models of rhinovirus-induced disease and exacerbation of allergic airway inflammation. Nat. Med. 14:199-204. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
