

Clinical and laboratory update on blastomycosis
- PMID: 20375357
- PMCID: PMC2863359
- DOI: 10.1128/CMR.00056-09
Clinical and laboratory update on blastomycosis
Abstract
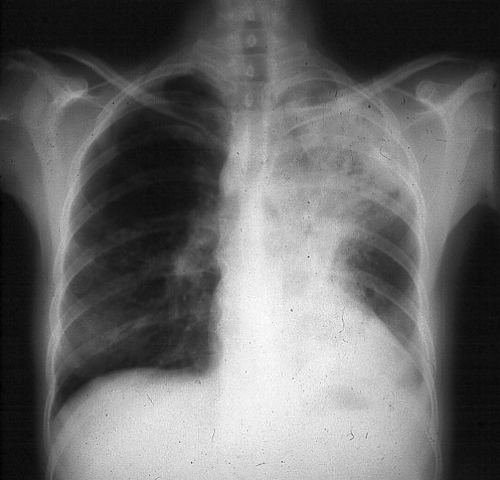
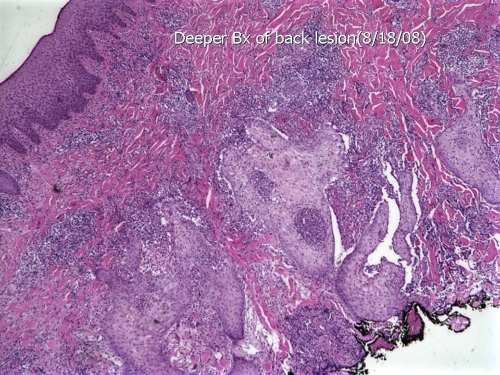
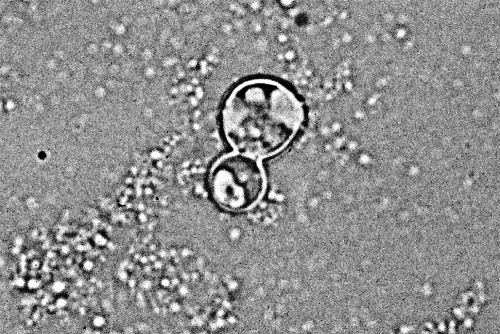
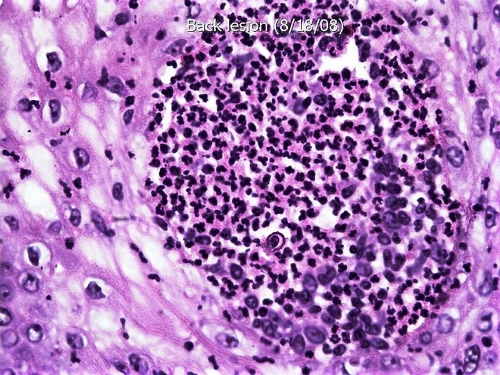
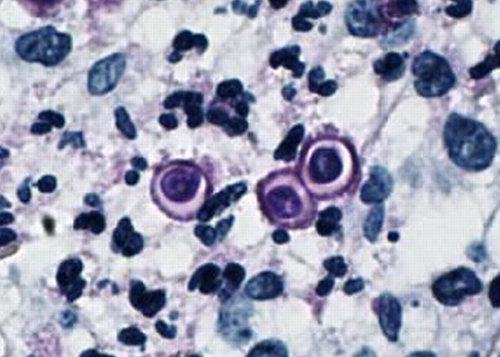
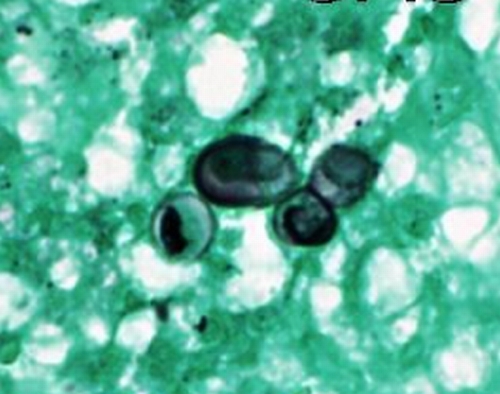
Blastomycosis is endemic in regions of North America that border the Great Lakes and the St. Lawrence River, as well as in the Mississippi River and Ohio River basins. Men are affected more often than women and children because men are more likely to participate in activities that put them at risk for exposure to Blastomyces dermatitidis. Human infection occurs when soil containing microfoci of mycelia is disturbed and airborne conidia are inhaled. If natural defenses in the alveoli fail to contain the infection, lymphohematogenous dissemination ensues. Normal host responses generate a characteristic pyogranulomatous reaction. The most common sites of clinical disease are the lung and skin; osseous, genitourinary, and central nervous system manifestations follow in decreasing order of frequency. Blastomycosis is one of the great mimickers in medicine; verrucous cutaneous blastomycosis resembles malignancy, and mass-like lung opacities due to B. dermatitidis often are confused with cancer. Blastomycosis may be clinically indistinguishable from tuberculosis. Diagnosis is based on culture and direct visualization of round, multinucleated yeast forms that produce daughter cells from a single broad-based bud. Although a long course of amphotericin B is usually curative, itraconazole is also highly effective and is the mainstay of therapy for most patients with blastomycosis.
Figures





References
-
- Abernathy, R. S. 1959. Clinical manifestations of pulmonary blastomycosis. Ann. Intern. Med. 51:707-727. - PubMed
-
- Abernathy, R. S. 1967. Amphotericin therapy of North American blastomycosis. Antimicrob. Agents Chemother. 3:208-211. - PubMed
-
- Amini, M., W. E. Shams, T. Barklow, and F. A. Sarubbi. 2007. A 45-year-old man with fever and adult respiratory distress syndrome. Clin. Infect. Dis. 44:566-567, 615-616. - PubMed
-
- Ashley, E. S. D., R. Lewis, J. S. Lewis, C. Martin, and D. Andes. 2006. Pharmacology of systemic antifungal agents. Clin. Infect. Dis. 43:S28-S39.
-
- Axelson, G. K., T. Giorgadze, and G. A. Youngberg. 2008. Evaluation of the use of Congo red staining in the differential diagnosis of Candida vs. various other yeast-form fungal organisms. J. Cutan. Pathol. 35:27-30. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
