

Integration of genetic, clinical, and INR data to refine warfarin dosing
- PMID: 20375999
- PMCID: PMC2858245
- DOI: 10.1038/clpt.2010.13
Integration of genetic, clinical, and INR data to refine warfarin dosing
Abstract
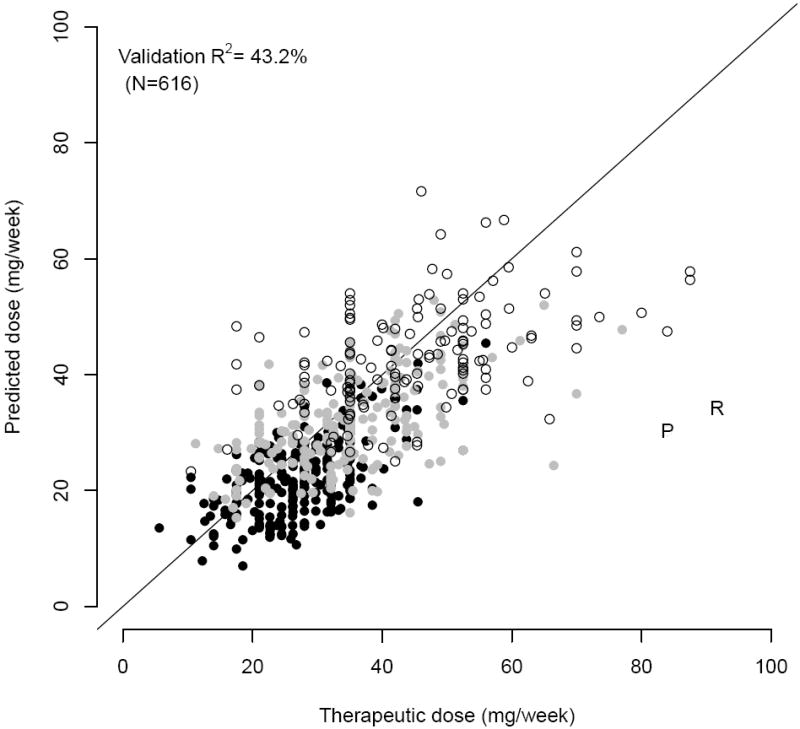
Well-characterized genes that affect warfarin metabolism (cytochrome P450 (CYP) 2C9) and sensitivity (vitamin K epoxide reductase complex 1 (VKORC1)) explain one-third of the variability in therapeutic dose before the international normalized ratio (INR) is measured. To determine genotypic relevance after INR becomes available, we derived clinical and pharmacogenetic refinement algorithms on the basis of INR values (on day 4 or 5 of therapy), clinical factors, and genotype. After adjusting for INR, CYP2C9 and VKORC1 genotypes remained significant predictors (P < 0.001) of warfarin dose. The clinical algorithm had an R(2) of 48% (median absolute error (MAE): 7.0 mg/week) and the pharmacogenetic algorithm had an R(2) of 63% (MAE: 5.5 mg/week) in the derivation set (N = 969). In independent validation sets, the R(2) was 26-43% with the clinical algorithm and 42-58% when genotype was added (P = 0.002). After several days of therapy, a pharmacogenetic algorithm estimates the therapeutic warfarin dose more accurately than one using clinical factors and INR response alone.
Conflict of interest statement
Figures
References
-
- Budnitz DS, Pollock DA, Weidenbach KN, et al. National surveillance of emergency department visits for outpatient adverse drug events. Jama. 2006 Oct 18;296:1858–66. - PubMed
-
- Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med. 2007 Jul 9;167:1414–9. - PubMed
-
- Lindh JD, Holm L, Dahl ML, et al. Incidence and predictors of severe bleeding during warfarin treatment. J Thromb Thrombolysis. 2008 Apr;25:151–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
