

Implicit value judgments in the measurement of health inequalities
- PMID: 20377756
- PMCID: PMC2888011
- DOI: 10.1111/j.1468-0009.2010.00587.x
Implicit value judgments in the measurement of health inequalities
Abstract
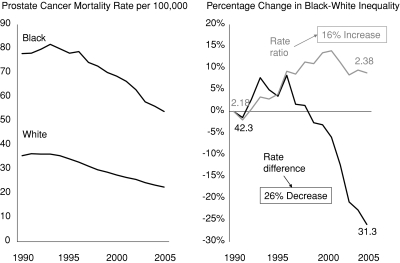
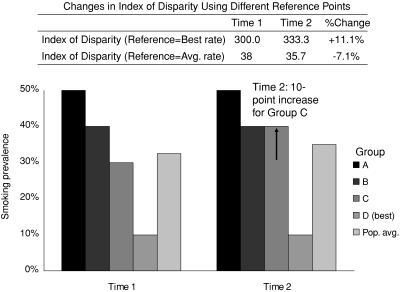
Context: Quantitative estimates of the magnitude, direction, and rate of change of health inequalities play a crucial role in creating and assessing policies aimed at eliminating the disproportionate burden of disease in disadvantaged populations. It is generally assumed that the measurement of health inequalities is a value-neutral process, providing objective data that are then interpreted using normative judgments about whether a particular distribution of health is just, fair, or socially acceptable.
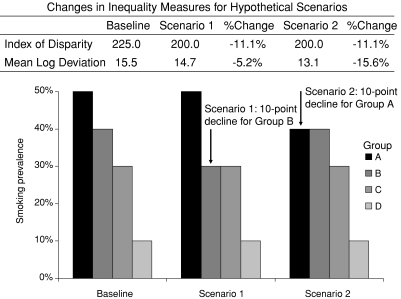
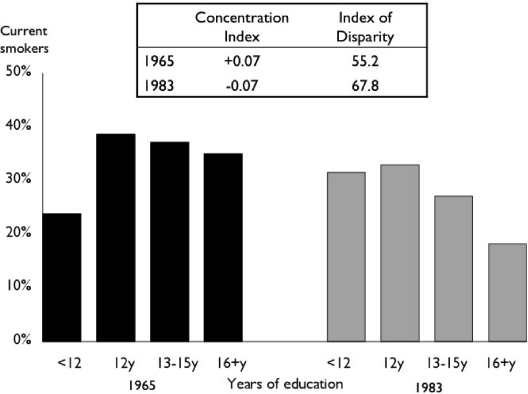
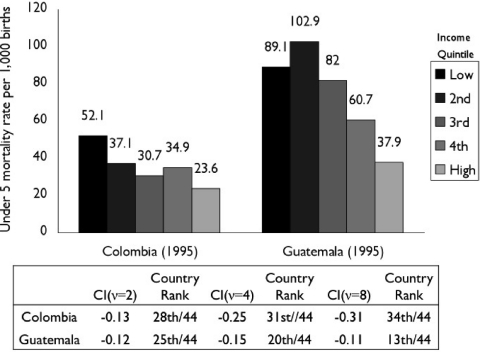
Methods: We discuss five examples in which normative judgments play a role in the measurement process itself, through either the selection of one measurement strategy to the exclusion of others or the selection of the type, significance, or weight assigned to the variables being measured.
Findings: Overall, we find that many commonly used measures of inequality are value laden and that the normative judgments implicit in these measures have important consequences for interpreting and responding to health inequalities.
Conclusions: Because values implicit in the generation of health inequality measures may lead to radically different interpretations of the same underlying data, we urge researchers to explicitly consider and transparently discuss the normative judgments underlying their measures. We also urge policymakers and other consumers of health inequalities data to pay close attention to the measures on which they base their assessments of current and future health policies.
Figures
Comment in
-
Measuring health-related differences among subgroups within populations.Milbank Q. 2010 Mar;88(1):1-3. doi: 10.1111/j.1468-0009.2010.00586.x. Milbank Q. 2010. PMID: 20377755 Free PMC article. No abstract available.
-
On the choice of absolute or relative inequality measures.Milbank Q. 2010 Dec;88(4):616-22; discussion 623-7. doi: 10.1111/j.1468-0009.2010.00614.x. Milbank Q. 2010. PMID: 21166871 Free PMC article.
References
-
- Atkinson AB. On the Measurement of Inequality. Journal of Economic Theory. 1970;2:244–63.
-
- Cowell FA. Measurement of Inequality. In: Atkinson AB, Bourguignon F, editors. Handbook of Income Distribution. Amsterdam: Elsevier; 2000. pp. 87–166.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
