

Association between length of storage of red blood cell units and outcome of critically ill children: a prospective observational study
- PMID: 20377853
- PMCID: PMC2887178
- DOI: 10.1186/cc8953
Association between length of storage of red blood cell units and outcome of critically ill children: a prospective observational study
Abstract
Introduction: Transfusion is a common treatment in pediatric intensive care units (PICUs). Studies in adults suggest that prolonged storage of red blood cell units is associated with worse clinical outcome. No prospective study has been conducted in children. Our objectives were to assess the clinical impact of the length of storage of red blood cell units on clinical outcome of critically ill children.
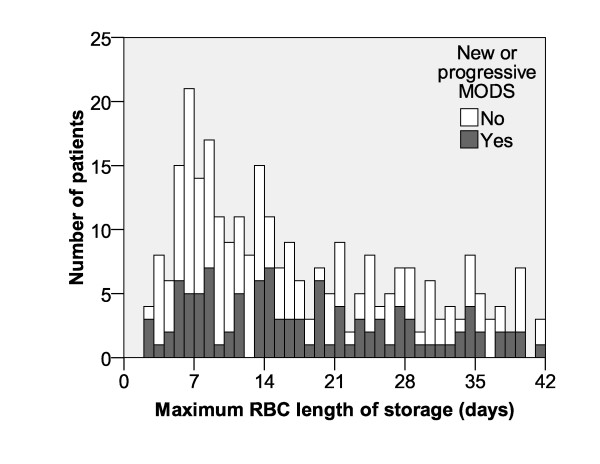
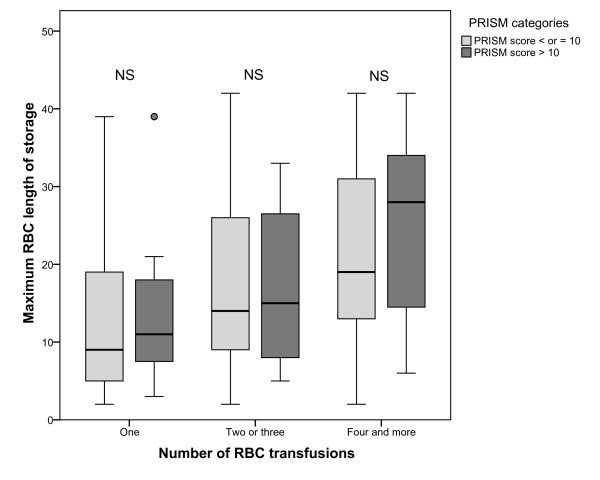
Methods: Prospective, observational study conducted in 30 North American centers, in consecutive patients aged <18 years with a stay >or= 48 hours in a PICU. The primary outcome measure was the incidence of multiple organ dysfunction syndrome after transfusion. The secondary outcomes were 28-day mortality and PICU length of stay. Odds ratios were adjusted for gender, age, number of organ dysfunctions at admission, total number of transfusions, and total dose of transfusion, using a multiple logistic regression model.
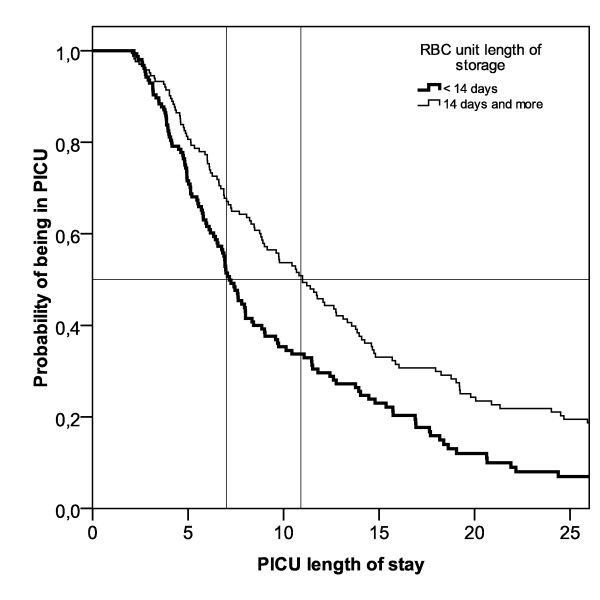
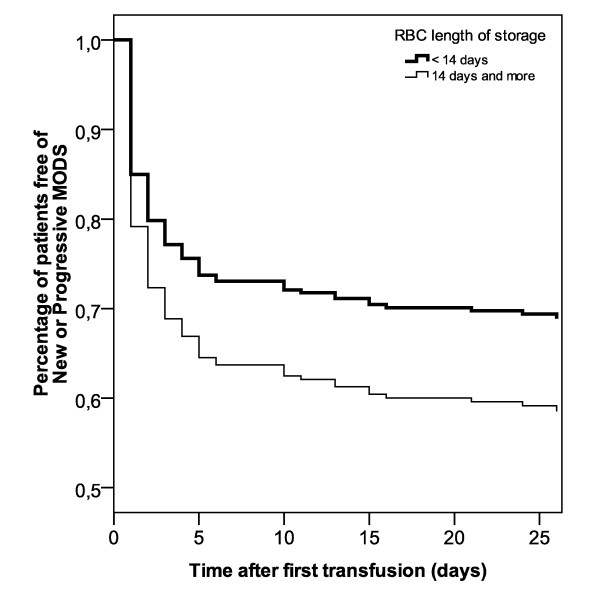
Results: The median length of storage was 14 days in 296 patients with documented length of storage. For patients receiving blood stored >or= 14 days, the adjusted odds ratio for an increased incidence of multiple organ dysfunction syndrome was 1.87 (95% CI 1.04;3.27, P = 0.03). There was also a significant difference in the total PICU length of stay (adjusted median difference +3.7 days, P < 0.001) and no significant change in mortality.
Conclusions: In critically ill children, transfusion of red blood cell units stored for >or= 14 days is independently associated with an increased occurrence of multiple organ dysfunction syndrome and prolonged PICU stay.
Figures
Comment in
-
Should fresh blood be recommended for intensive care patients?Crit Care. 2010;14(3):158. doi: 10.1186/cc9011. Epub 2010 May 20. Crit Care. 2010. PMID: 20565831 Free PMC article.
References
-
- Corwin HL, Gettinger A, Pearl RG, Fink MP, Levy MM, Abraham E, MacIntyre NR, Shabot MM, Duh MS, Shapiro MJ. The CRIT Study: Anemia and blood transfusion in the critically ill--current clinical practice in the United States. Crit Care Med. 2004;32:39–52. doi: 10.1097/01.CCM.0000104112.34142.79. - DOI - PubMed
-
- Bateman S, Lacroix J, Boven K, Forbes P, Barton R, Thomas N, Jacobs B, Markovitz B, Goldstein B, Hanson J, Li H, Randolph A. Anemia, blood loss, and blood transfusions in North American children in the intensive care unit. Am J Resp Crit Care Med. 2008;178:26–33. doi: 10.1164/rccm.200711-1637OC. - DOI - PubMed
-
- Spinella PC, Perkins JG, Grathwohl KW, Beekley AC, Niles SE, McLaughlin DF, Wade CE, Holcomb JB. Effect of plasma and red blood cell transfusions on survival in patients with combat related traumatic injuries. J Trauma. 2008;64:S69–77. doi: 10.1097/TA.0b013e318160ba2f. discussion S77-68. - DOI - PubMed
-
- Sauaia A, Moore FA, Moore EE, Haenel JB, Read RA, Lezotte DC. Early predictors of postinjury multiple organ failure. Arch Surg. 1994;129:39–45. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
