

Periprocedural bleeding complications of brain AVM embolization with Onyx
- PMID: 20377979
- PMCID: PMC3277965
- DOI: 10.1177/159101991001600106
Periprocedural bleeding complications of brain AVM embolization with Onyx
Erratum in
- Interv Neuroradiol. 2010 Jun;16(2):213
Abstract
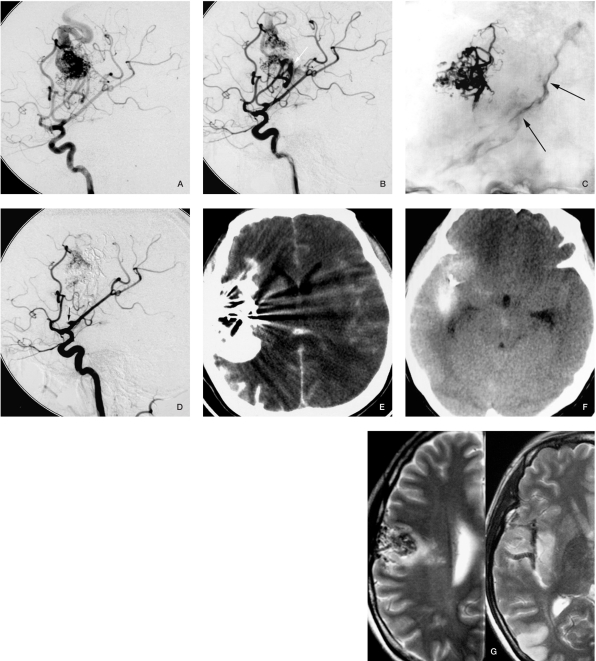
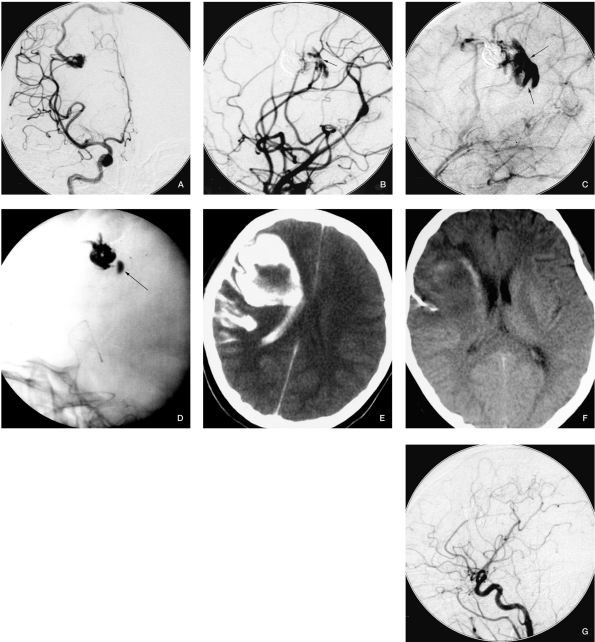
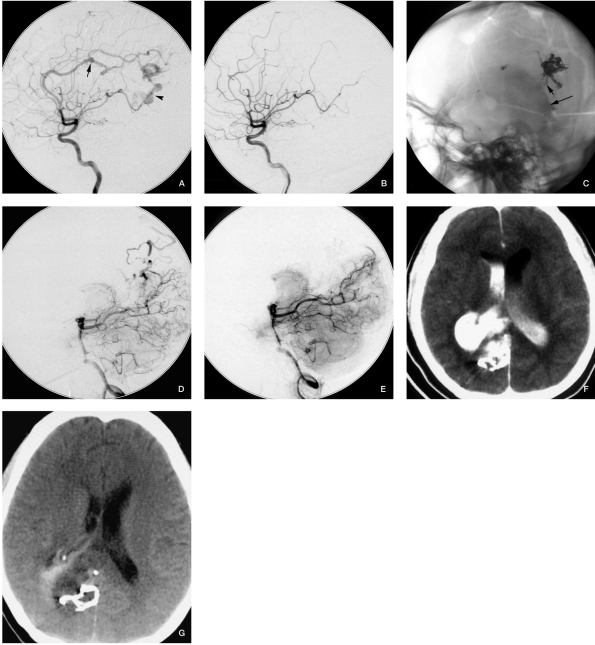
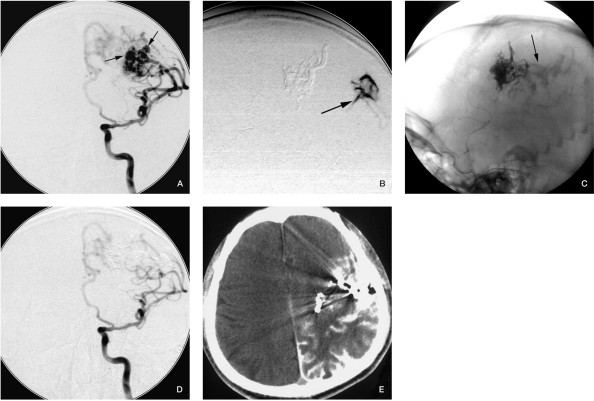
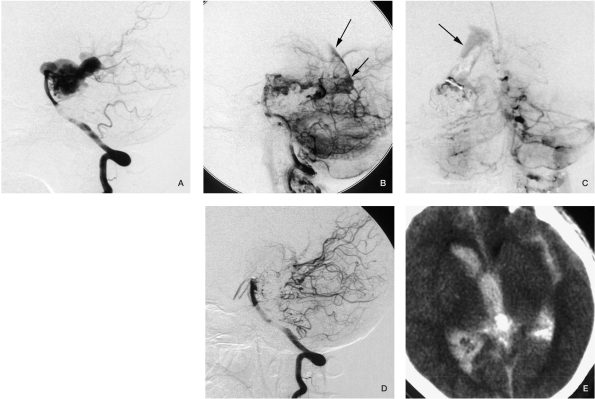
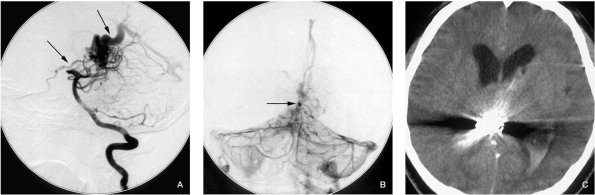
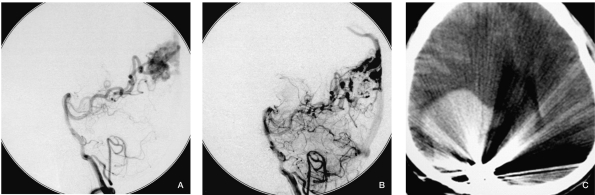
The advent of Onyx has provided a new method for neurointerventional therapists to treat brain AVMs. Although some retrospective studies have reported complications for AVM embolization with Onyx, periprocedural bleeding complications with Onyx embolization have not yet been described in detail. The aim of this retrospective study was to analyze the factors of Onyx-related bleeding complications and to find a way to avoid and manage these complications.From January 2003, patients with AVMs recruited in our institution started to be treated by Onyx embolization. From January 2007 to July 2009, 143 consecutive interventions were performed in 126 patients using flow-independent microcatheters and Onyx as embolic agents. Seven patients encountered bleeding complications (5.4% per patients and 4.7% per procedures) during or after the endovascular procedures. Among them, five bleeding episodes occurred during procedures, the other two after procedures. Details of the seven patients' clinical presentations, imaging presentations, speculative reasons and management of these complications were recorded. Follow-up data, including postoperative course, clinical symptoms and duration of follow-up were documented. The five active bleedings discovered in procedures were managed in time, and the patients recovered without any new neurological symptoms compared with preoperation. However, of the two bleeding episodes that occurred after interventional procedures, one was detected half an hour later: the patient was remained comatose two months later after resection of right occipital hematoma; the other who encountered intraventricular and midbrain hemorrhage was treated conservatively and suffered Parinaud syndrome and hemianesthesia.
Conclusion: Periprocedural bleeding of AVMs embolization is considered a severe and devastating complication. The clinical course and prognosis of bleeding mostly depends on prompt detection and management. Interventional embolization is an effective method to manage bleeding during procedures, and the detection of risk factors and imaging signs of bleeding is extremely important.
Figures
Similar articles
-
Neurological morbidity and mortality associated with the endovascular treatment of cerebral arteriovenous malformations before and during the Onyx era.J Neurosurg. 2015 Jun;122(6):1492-7. doi: 10.3171/2015.2.JNS131368. Epub 2015 Mar 27. J Neurosurg. 2015. PMID: 25816081
-
Complication risk of endovascular embolization for cerebral arteriovenous malformation.Eur J Radiol. 2011 Dec;80(3):776-9. doi: 10.1016/j.ejrad.2010.09.024. Epub 2010 Oct 14. Eur J Radiol. 2011. PMID: 20950972
-
Multimodality treatment of brain arteriovenous malformations with microsurgery after embolization with onyx: single-center experience and technical nuances.Neurosurgery. 2008 Jun;62(6):1213-25; discussion 1225-6. doi: 10.1227/01.neu.0000333293.74986.e5. Neurosurgery. 2008. PMID: 18824988
-
Delayed Migration of Onyx Embolic Agent after Preoperative Embolization of an Arteriovenous Malformation in a Pediatric Patient: A Case Report and Review of the Literature.Pediatr Neurosurg. 2023;58(1):45-52. doi: 10.1159/000529629. Epub 2023 Feb 13. Pediatr Neurosurg. 2023. PMID: 36780879 Review.
-
Intracerebral hemorrhage following endovascular embolization of brain arteriovenous malformation with a combination of Onyx and n-butyl cyanoacrylate: a case report.Clin Imaging. 2012 Jul-Aug;36(4):375-8. doi: 10.1016/j.clinimag.2011.09.003. Epub 2012 Jun 8. Clin Imaging. 2012. PMID: 22726978 Review.
Cited by
-
Microcatheter entrapment retrieval from Onyx embolization in brain arteriovenous malformations: A technical note.Interv Neuroradiol. 2015 Oct;21(5):620-3. doi: 10.1177/1591019915583226. Epub 2015 Jul 31. Interv Neuroradiol. 2015. PMID: 26232252 Free PMC article.
-
Intra- and post-operative acute hemorrhagic complications of Onyx embolization of brain arteriovenous malformations: A single-center experience.Front Neurol. 2022 Sep 23;13:974954. doi: 10.3389/fneur.2022.974954. eCollection 2022. Front Neurol. 2022. PMID: 36212665 Free PMC article.
-
FLAIR hyperintense vessels on MRI post brain arteriovenous malformation embolization: A novel finding associated with post-procedure intraparenchymal hemorrhage.Interv Neuroradiol. 2025 Feb;31(1):17-23. doi: 10.1177/15910199221146585. Epub 2022 Dec 26. Interv Neuroradiol. 2025. PMID: 36572982 Free PMC article.
-
Assessment of periprocedural hemodynamic changes in arteriovenous malformation vessels by endovascular dual-sensor guidewire.Interv Neuroradiol. 2015 Feb;21(1):101-7. doi: 10.15274/inr-2014-10096. Interv Neuroradiol. 2015. PMID: 25934783 Free PMC article.
-
One-stop hybrid operation versus microsurgery for treating brain arteriovenous malformation in children-a retrospective case series.Transl Pediatr. 2024 Jul 31;13(7):1051-1060. doi: 10.21037/tp-24-68. Epub 2024 Jul 18. Transl Pediatr. 2024. PMID: 39144421 Free PMC article.
References
-
- Biondi A, Le Jean L, et al. Fatal hemorrhagic complication following endovascular treatment of a cerebral arteriovenous malformation. Case report and review of the literature. J Neuroradiol. 2006;33(2):96–104. - PubMed
-
- Hartmann A, Stapf C, et al. Determinants of neurological outcome after surgery for brain arteriovenous malformation. Stroke. 2000;31:2361–2364. - PubMed
-
- Hartmann A, Pile-Spellman J, et al. Risk of endovascular treatment of brain arteriovenous malformations. Stroke. 2002;33:1816–1820. - PubMed
-
- Ledezma CJ, Hoh BL, et al. Complications of cerebral arteriovenous malformation embolization: multivariate analysis of predictive factors. Neurosurgery. 2006;58(4):602–611. discussion 602-611. - PubMed
-
- Stapf C, Mast H, et al. Predictors of hemorrhage in patients with untreated brain arteriovenous malformation. Neurology. 2006;66:1350–1355. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
