

Emphasizing conformal avoidance versus target definition for IMRT planning in head-and-neck cancer
- PMID: 20378266
- PMCID: PMC2905233
- DOI: 10.1016/j.ijrobp.2009.09.062
Emphasizing conformal avoidance versus target definition for IMRT planning in head-and-neck cancer
Abstract
Purpose: To describe a method for streamlining the process of elective nodal volume definition for head-and-neck (H&N) intensity-modulated radiotherapy (IMRT) planning.
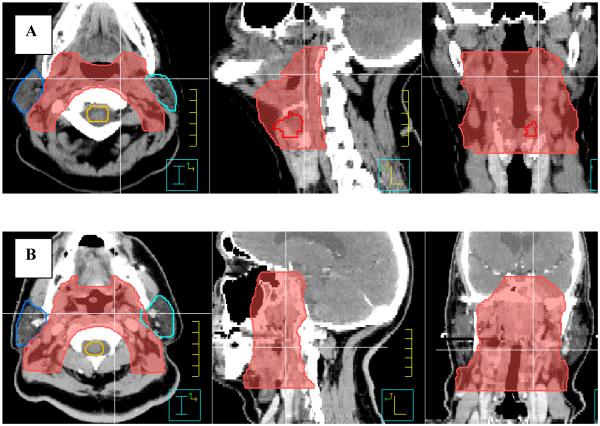
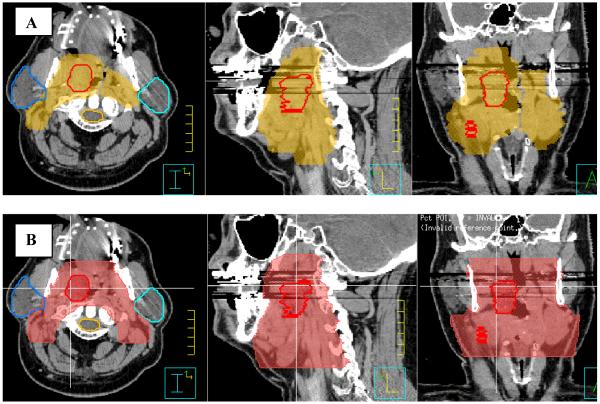
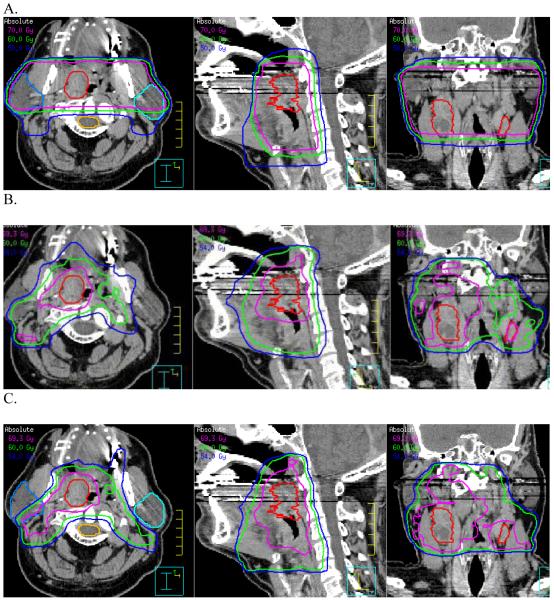
Methods and materials: A total of 20 patients who had undergone curative-intent RT for H&N cancer underwent comprehensive treatment planning using three distinct, plan design techniques: conventional three-field design, target-defined IMRT (TD-IMRT), and conformal avoidance IMRT (CA-IMRT). For each patient, the conventional three-field design was created first, thereby providing the "outermost boundaries" for subsequent IMRT design. In brief, TD-IMRT involved physician contouring of the gross tumor volume, high- and low-risk clinical target volume, and normal tissue avoidance structures on consecutive 1.25-mm computed tomography images. CA-IMRT involved physician contouring of the gross tumor volume and normal tissue avoidance structures only. The overall physician time for each approach was monitored, and the resultant plans were rigorously compared.
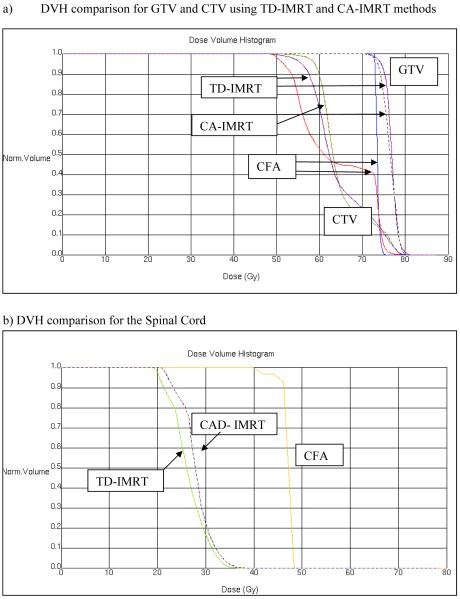
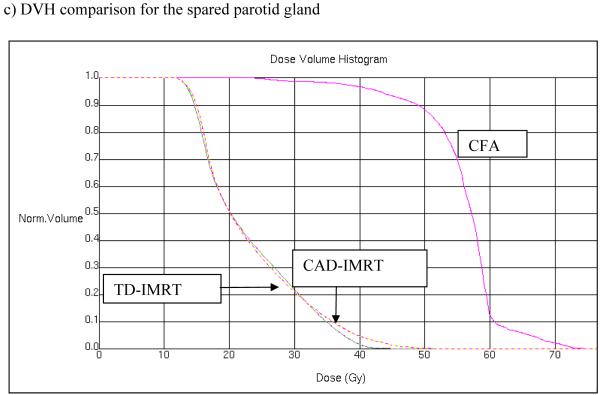
Results: The average physician working time for the design of the respective H&N treatment contours was 0.3 hour for the conventional three-field design plan, 2.7 hours for TD-IMRT, and 0.9 hour for CA-IMRT. Dosimetric analysis confirmed that the largest volume of tissue treated to an intermediate (50 Gy) and high (70 Gy) dose occurred with the conventional three-field design followed by CA-IMRT and then TD-IMRT. However, for the two IMRT approaches, comparable results were found in terms of salivary gland and spinal cord protection.
Conclusion: CA-IMRT for H&N treatment offers an alternative to TD-IMRT. The overall time for physician contouring was substantially reduced (approximately threefold), yielding a more standardized elective nodal volume. Because of the complexity of H&N IMRT target design, CA-IMRT might ultimately prove a safer and more reliable method to export to general radiation oncology practitioners, particularly those with limited H&N caseload experience.
(c) 2010 Elsevier Inc. All rights reserved.
Figures
References
-
- Eisbruch A, Kim HM, Terrell JE, Marsh LH, Dawson LA, Ship JA. Xerostomia and its predictors following parotid-sparing irradiation of head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2001;50:695–704. - PubMed
-
- Chao KS, Deasy JO, Markman J, Haynie J, Perez CA, Purdy JA, et al. A prospective study of salivary function sparing in patients with head-and-neck cancers receiving intensity-modulated or three-dimensional radiation therapy: initial results. Int J Radiat Oncol Biol Phys. 2001;49:907–916. - PubMed
-
- Nowak PJ, Wijers OB, Lagerwaard FJ, Levendag PC. A three-dimensional CT-based target definition for elective irradiation of the neck. Int J Radiat Oncol Biol Phys. 1999;45:33–39. - PubMed
-
- Martinez-Monge R, Fernandes PS, Gupta N, Gahbauer R. Cross-sectional nodal atlas: a tool for the definition of clinical target volumes in three-dimensional radiation therapy planning. Radiology. 1999;211:815–828. - PubMed
-
- Wijers OB, Levendag PC, Tan T, van Dieren EB, van Sornsen de Koste J, van der Est H, et al. A simplified CT-based definition of the lymph node levels in the node negative neck. Radiother Oncol. 1999;52:35–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
