

Left ventricular hypertrophy in new hemodialysis patients without symptomatic cardiac disease
- PMID: 20378644
- PMCID: PMC2863966
- DOI: 10.2215/CJN.07761109
Left ventricular hypertrophy in new hemodialysis patients without symptomatic cardiac disease
Abstract
Background and objectives: Although left ventricular hypertrophy (LVH) is a characteristic finding in hemodialysis (HD) populations, few risk factors for progressive LVH have been identified.
Design, setting, participants, & measurements: As part of a multinational, blinded, randomized, controlled trial that demonstrated no effect of hemoglobin targets on LV size, 596 incident HD patients, without symptomatic cardiac disease or cardiac dilation, had baseline echocardiograms within 18 months of starting dialysis and subsequently at 24, 48, and 96 weeks later. A wide array of baseline risk factors were assessed, as were BP and hemoglobin levels during the trial.
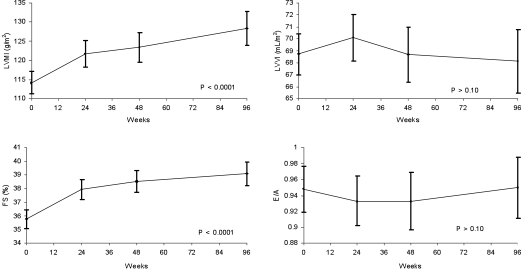
Results: The median age and duration of dialysis were 51.5 years and 9 months, respectively. LV mass index (LVMI) rose substantially during follow-up (114.2 g/m(2) at baseline, 121 at week 48, 123.4 at week 48, and 128.3 at week 96), as did fractional shortening, whereas LV volume (68.7, 70.1, 68.7, and 68.1 ml/m(2)) and E/A ratio remained unchanged. At baseline, the only multivariate associations of LVMI were gender and N terminal pro-B type natriuretic peptide. Comparing first and last echocardiograms in those without LVH at baseline, independent predictors of increase in LVMI were higher time-integrated systolic BP and cause of ESRD. An unadjusted association between baseline LVMI and subsequent cardiovascular events or death was eliminated by adjusting for age, diabetes, systolic BP, and N terminal pro-B type natriuretic peptide.
Conclusions: Progressive concentric LVH and hyperkinesis occur in HD patients, which is partly explained by hypertension but not by a wide array of potential risk factors, including anemia.
Figures
References
-
- Foley RN, Parfrey PS, Harnett JD, Kent GM, Martin CJ, Murray DC, Barre PE: Clinical and echocardiographic disease in patients starting end-stage renal disease therapy. Kidney Int 47: 186– 192, 1995 - PubMed
-
- Parfrey PS, Foley RN, Harnett JD, Kent GM, Murray DC, Barre PE: Outcome and risk factors for left ventricular disorders in chronic uraemia. Nephrol Dial Transplant 11: 1277– 1285, 1996 - PubMed
-
- Foley RN, Parfrey PS, Kent GM, Harnett JD, Murray DC, Barre PE: Long-term evolution of cardiomyopathy in dialysis patients. Kidney Int 54: 1720– 1725, 1998 - PubMed
-
- Parfrey PS, Foley RN, Wittreich BH, Sullivan DJ, Zagari MJ, Frei D: Double-blind comparison of full and partial anemia correction in incident hemodialysis patients without symptomatic heart disease. J Am Soc Nephrol 16: 2180– 2189, 2005 - PubMed
-
- Foley RN, Parfrey PS, Kent GM, Harnett JD, Murray DC, Barre PE: Serial change in echocardiographic parameters and cardiac failure in end-stage renal disease. J Am Soc Nephrol 11: 912– 916, 2000 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
