

Advances in diagnostic bronchoscopy
- PMID: 20378726
- PMCID: PMC3159074
- DOI: 10.1164/rccm.201002-0186CI
Advances in diagnostic bronchoscopy
Abstract
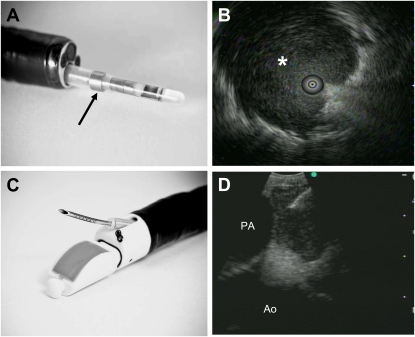
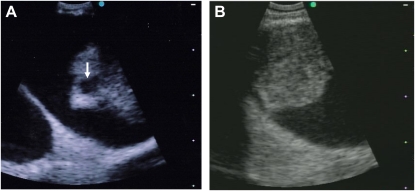
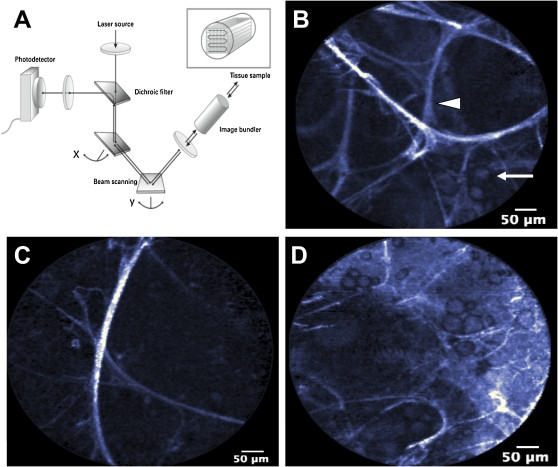
Diagnostic bronchoscopy has undergone two major paradigm shifts in the last 40 years. First, the advent of flexible bronchoscopy gave chest physicians improved access to the tracheobronchial tree with a rapid learning curve and greater patient comfort compared with rigid bronchoscopy. The second paradigm shift has evolved over the last 5 years with the proliferation of new technologies that have significantly enhanced the diagnostic capabilities of flexible bronchoscopy compared with traditional methods. At the forefront of these new technologies is endobronchial ultrasound. In its various forms, endobronchial ultrasound has improved diagnostic yield for pulmonary masses, nodules, intrathoracic adenopathy, and disease extent, thereby reducing the need for more invasive surgical interventions. Various navigational bronchoscopy systems have become available to increase flexible bronchoscope access to small peripheral pulmonary lesions. Furthermore, various modalities of airway assessment, including optical microscopic imaging technologies, may play significant roles in the diagnosis of a variety of pulmonary diseases in the future. Finally, the combination of new diagnostic bronchoscopy technologies and novel approaches in molecular analysis and biomarker assessment hold promise for enhanced diagnosis and personalized management of many pulmonary disorders. In this review, we provide a contemporary review of diagnostic bronchoscopy developments over the past decade.
Figures
References
-
- Yeow KM, Su IH, Pan KT, Tsay PK, Lui KW, Cheung YC, Chou AS. Risk factors of pneumothorax and bleeding: multivariate analysis of 660 CT-guided coaxial cutting needle lung biopsies. Chest 2004;126:748–754. (See comment). - PubMed
-
- Ohno Y, Hatabu H, Takenaka D, Higashino T, Watanabe H, Ohbayashi C, Sugimura K. CT-guided transthoracic needle aspiration biopsy of small (≤20 mm) solitary pulmonary nodules. AJR Am J Roentgenol 2003;180:1665–1669. - PubMed
-
- Schreiber G, McCrory DC. Performance characteristics of different modalities for diagnosis of suspected lung cancer: summary of published evidence. Chest 2003;123:115S–128S. - PubMed
-
- Baaklini WA, Reinoso MA, Gorin AB, Sharafkaneh A, Manian P. Diagnostic yield of fiberoptic bronchoscopy in evaluating solitary pulmonary nodules. Chest 2000;117:1049–1054. - PubMed
-
- Paone G, Nicastri E, Lucantoni G, Dello Iacono R, Battistoni P, D'Angeli AL, Galluccio G. Endobronchial ultrasound-driven biopsy in the diagnosis of peripheral lung lesions. Chest 2005;128:3551–3557. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
