

doi: 10.1155/2009/634567.
Epub 2010 Mar 31.
Use of cone beam computed tomography in endodontics
Affiliations
- PMID: 20379362
- PMCID: PMC2850139
- DOI: 10.1155/2009/634567
Item in Clipboard
Use of cone beam computed tomography in endodontics
Int J Dent.
2009.
Abstract
Cone Beam Computed Tomography (CBCT) is a diagnostic imaging modality that provides high-quality, accurate three-dimensional (3D) representations of the osseous elements of the maxillofacial skeleton. CBCT systems are available that provide small field of view images at low dose with sufficient spatial resolution for applications in endodontic diagnosis, treatment guidance, and posttreatment evaluation. This article provides a literature review and pictorial demonstration of CBCT as an imaging adjunct for endodontics.
Figures
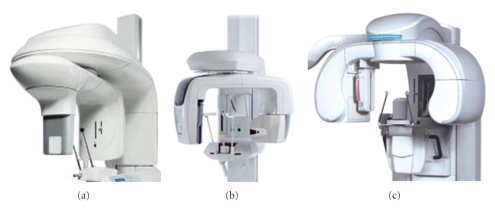
Examples of hybrid CBCT units. (a) KODAK Dental Imaging 9000 3D, (b) Veraviewepocs 3D, and (c) Picasso Trio.
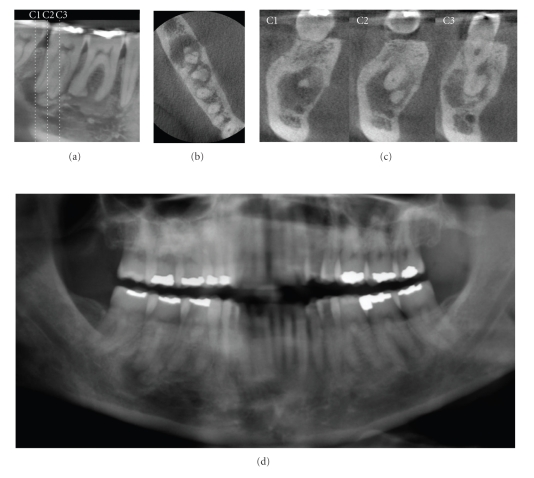
A 52-year-old Caucasian female was referred for assessment of multiple periapical areas associated with the mandibular right first and second molars. Curved planar (a), axial (b), and correlated multiple cross-sectional (c) images are shown. There are areas of mixed central opacity and peripheral radiolucency associated with the apices of the teeth; however no expansion, tooth resorption, or displacement is evident. Hypercementosis is observed on the distal root of the first molar. On clinical examination, all teeth in this quadrant tested vital. Based on a working diagnosis of florid cemento-osseous dysplasia, an additional digital panoramic radiograph ((d) cropped panoramic image) was performed and revealed similar bony patterns in the left posterior maxilla and mandible. Management of this patient comprised a 6-month recall comparison of focused CBCT images to judge the progression of the lesion.
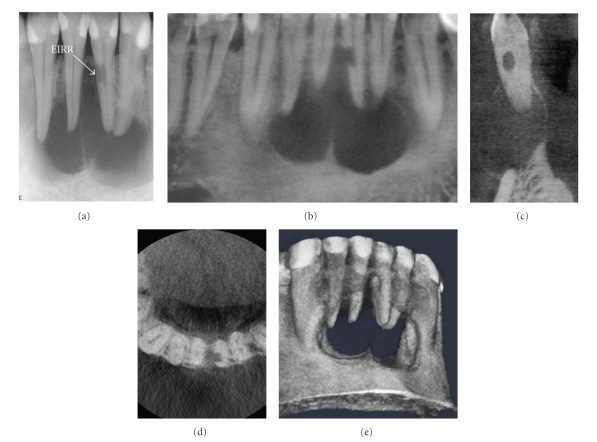
After suffering a traumatic blow from a soccer ball six years earlier, a 28-year-old male presented with a soft, convex-shaped indurated buccal and lingual swelling in the mandibular symphyseal region. A periapical image (a) showed a large, multilocular lesion. External inflammatory root resorption (EIRR) was noted on the mandibular left lateral incisor. All four mandibular anterior teeth tested nonvital. CBCT images ((b) curved planar, (c) cross-sectional, (d) axial, (e) 3D reconstruction) showed that the resorptive lesion was extended from the root canal space to the periodontal membrane, necessitating repair or extraction; no exploratory procedure was necessary to determine the extent of the defect.
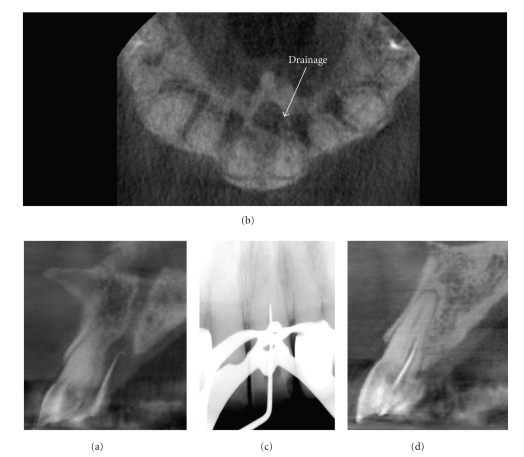
A 79-year-old male was referred for endodontic treatment of the maxillary left central incisor after a palatal sinus tract was noted. CBCT imaging was initially performed with a gutta percha cone marker inserted into the sinus tract to determine the source of the infection. Sagittal images (a) demonstrated that the lesion terminated at the periapex of the maxillary left central incisor after coursing through the incisive canal whereas drainage was visible on the axial image (b). Perioperatively, only the mesiodistal direction could be determined on conventional intraoral periapical radiography (c) and treatment suspended when the explorer reached 17 mm because of the danger of perforation in the facial or palatal direction. Subsequent cross-sectional perioperative CBCT imaging (d) with an intracanal gutta percha marker indicated that the initial access preparation was directed palatally. Correction of the access facially resulted in gaining access to the apical terminus; treatment was completed without complication.

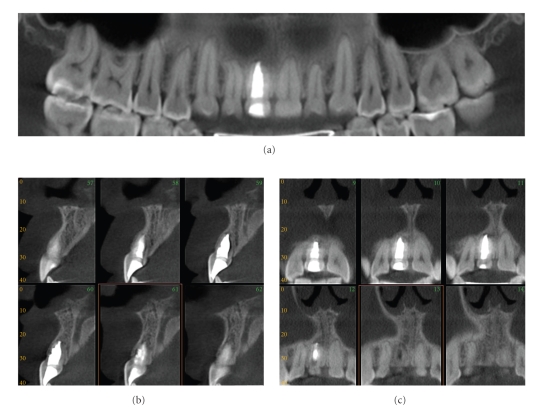
Treatment of large destructive lesions associated with pulpal pathosis benefit from 3D imaging providing better visualization of the spatial relationships of the tooth to anatomic landmarks and canal morphology. This patient presented with mild dysthesia of the right mandibular dentition. Conventional periapical imaging (a) demonstrated a large apical and mesial ill-defined rarefaction associated with the right mandibular second molar in close proximity to the inferior alveolar nerve. CBCT images ((b) sagittal, (c) cross-sectional, (d) axial) demonstrate the proximity of the lesion to the mandibular canal (MC). Therefore during treatment great care was taken to prevent obturation material extrusion past the apical terminus and possible traumatization of the IAN. Additional parasagittal CBCT images document the progression of healing at 6 months (e). In addition digital subtraction composite 3D imaging at 6 months (f) provides three-dimensional visualization of healing. (Data acquired at 0.076 mm resolution on an KODAK Dental Imaging 9000 DS (Dental Imaging/Practiceworks Atlanta, GA, USA) and 3D subtraction composite reformatted using InVivo Dental (Anatomage, San Jose, CA)).
A female patient presented with a twenty-year history of mostly continuous, unilateral, poorly localized severe aching of the maxillary left quadrant. The pain was not associated with sensory loss or other physical signs and pulp tests, and conventional imaging studies were within normal limits. Clinically there was no cessation of pain after administration of local anesthetic. This neuropathic pain syndrome, initially termed atypical facial pain, is more recently known as persistent idiopathic facial pain (PIFP). PIFP refers to pain along the territory of the trigeminal nerve that does not fit the classic presentation of other cranial neuralgias. Diagnostically challenging, PIFP is frequently misdiagnosed and is often attributed by patients to dental procedures, facial trauma, and rarely, by some clinicians, as Neuralgia-Inducing Cavitational Osteonecrosis (NICO). Dynamic visualization of sequential curved planar parasagittal CBCT-reformatted images at 0.076 mm thickness (a) confirmed the absence of obvious pathosis of odontogenic origin as diagnosed from the original intraoral periapical of the region (b). Note the radiolucent area within the coronal portion of the first molar under the radiopaque disto-occlusal restorative material; this represents a streak artifact due to “photostarvation” in the horizontal plane due to the attenuation of adjacent amalgam and radiopaque material and subsequent reduction in available data for image reconstruction. A negative CBCT imaging finding is often very reassuring for these unfortunate patients who often question a nonodontogenic diagnosis. Psychiatric symptoms of depression and anxiety are prevalent in this population and compound the diagnostic conundrum.
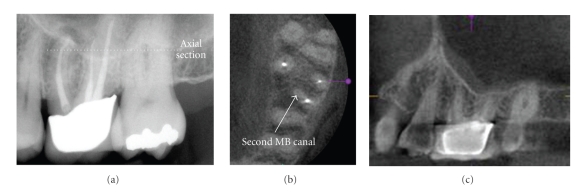
Maxillary first and second molars often present treatment challenges because of the frequent presence of mesioaccessory (mb2) canals. On initial periapical radiographic examination of this previously treated maxillary left first molar, no mb2 canal was detected; however a periapical lesion is seen (a). Note the overlap of the interproximal contacts between the molars indicating a geometric distortion in the horizontal plane. CBCT imaging ((b) 0.076 mm axial and (c) 0.076 parasagittal) clearly demonstrates an additional canal that was not previously treated.
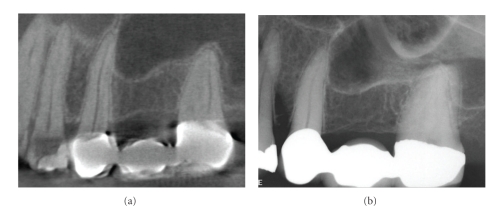
On conventional intraoral periapical radiography periapical mucositis (PM) presents as a relatively radiopaque, soft-tissue, dome-shaped lesion localized to the apex of a maxillary posterior tooth and projecting into the floor of the maxillary sinus. Most are indistinguishable from mucosal lesions of intrinsic sinus origin such as antral mucosal pseudocysts (see Figure 9). While clinically asymptomatic, they are usually associated with necrotic or failing root canal-filled teeth. PM is a localized mucosal thickening of the sinus membrane, secondary to a breach of periradicular inflammation, and will resolve after successful endodontic treatment. This patient gave a history of persistent left side pain over the maxillary molar region of 4-month duration. Treatment for sinusitis did not relieve the symptoms. Panoramic and intraoral dental radiology did not reveal a cause. Coronal CBCT imaging (a) demonstrates acute sinusitis bilaterally with 50% to 70% opacification and previous uncinectomy and antrostomy (as evidenced by the loss of the superior medial wall of the right sinus) of the right sinus, whereas the left sinus shows thickened mucosal lining with a dome-shaped soft tissue lesion overlying the roots of the restored left maxillary first molar tooth. 5 mm reformatted panoramic (b) and 1 mm cross-sectional (c) reconstructions of the maxillary left first molar show periapical lesional penetration and communication with the floor of the sinus in this region. Data acquired on an iCAT, Imaging Sciences International, Hatfield, PA USA at 0.3 mm resolution and reformatted using InVivo Dental, Anatomage, San Jose, CA.
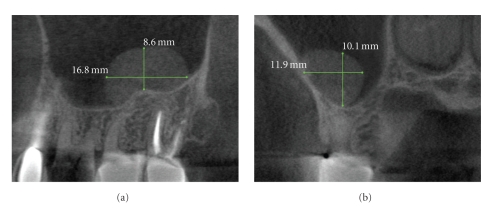
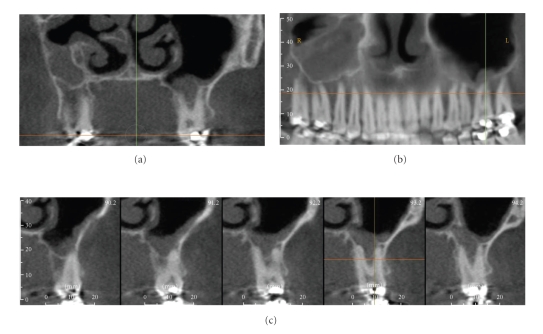
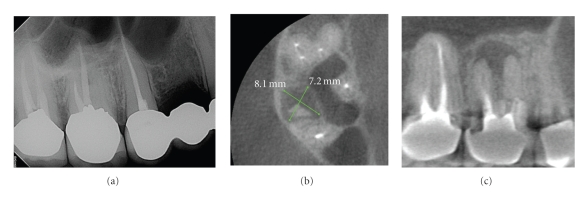
Antral mucosal pseudocysts, also called mucus retention cysts, are a relatively common localized dome-shaped antral mucosal swelling, often of allergic origin and while they can occur anywhere in the sinus present diagnostic challenges when associated with the floor of the maxillary sinus. CBCT imaging ((a) sagittal, (b) cross-sectional) can be useful in differentiating these lesions from periapical mucositis in that the former is usually not associated with disruption of the floor of the sinus and expansion superiorly from the apex of roots of adjacent teeth.
A periapical radiograph of the maxillary left first molar (a) shows an area of low density surrounding the mesial root with incomplete endodontic treatment. A contemporaneous CBCT parasagittal image (b) shows a chronic periradicular osteoperiostitis, or “halo lesion,” where the apical periodontitis has caused displacement of the periosteum but did not penetrate the antral floor. Three months after retreatment, CBCT imaging (c) demonstrates complete apical resolution.
This patient was referred for discomfort and swelling in the maxillary right quadrant. While an initial periapical radiograph (a) clearly demonstrated an untreated mesial root in the maxillary first molar, periradicular periodontitis was undetectable. CBCT images ((a) axial, (b) sagittal) clearly identify a large apical radiolucent lesion associated with the mesial root extending to the distobuccal root. The tooth was retreated and the symptoms subsided.
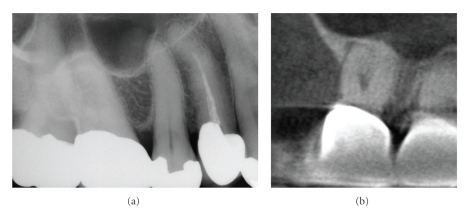
Difficulty in visualizing furcal and apical lesions with periapical radiography due to lack of coverage, anatomic superimposition, and geometric distortion is well established. The periapical radiograph (a) of the maxillary right second molar in an asymptomatic patient is unremarkable; however there is lack of coverage of the second molar posteriorly and marked superimposition of the distal root of the first molar over the mesial root of the second molar. The corresponding cropped sagittal CBCT image (b) of the second molar demonstrates a furcal radiolucency and associated periradicular periodontitis. Subsequent clinical investigation found this tooth to be nonvital.
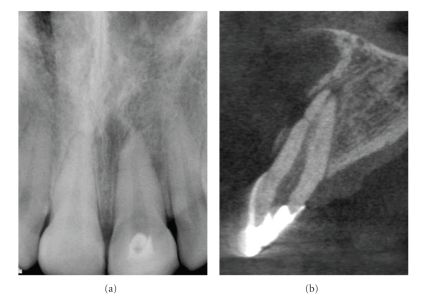
Traumatic injuries to the anterior dentition may result in a horizontal root fracture. Visualizing these fractures with periapical radiographs can be difficult as the beam must be in parallel alignment to the axis of the fracture. Conventional periapical image (a) shows horizontal radiolucent line separating the apical 1/3rd of the root. Note the loss of lamina dura and lateral radiolucency on the distal root surface adjacent to the horizontal radiolucency. Cross-sectional high-resolution (0.076 mm) image showing “V” shaped fracture and minimal displacement of the root segments. Note the loss of buccal cortical plate, widening of the buccal periodontal ligament space and periapical rarefaction.
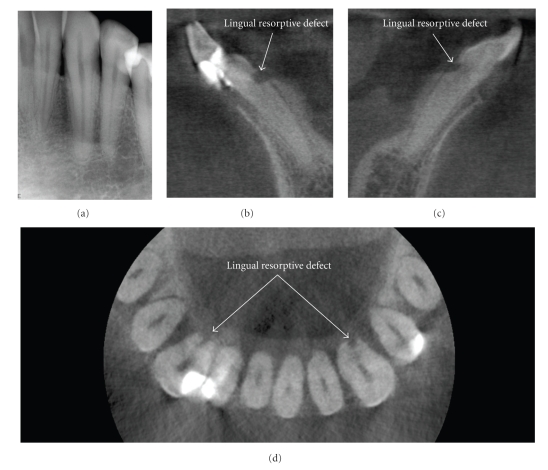
This patient was referred for endodontic revision of the mandibular right lateral incisor. Initial periapical radiographic examination of the mandibular anterior teeth including the left anterior (a) was unremarkable. Note the appearance of a large radiolucency at the on the distal surface of the left canine due to nonperpendicular X-ray beam projection of the distal curvature of the cervical margin. CBCT images ((b) right cross-sectional, (c) left cross-sectional, (d) axial) demonstrated an occult finding of early ERR on the mandibular left and right mandibular cuspids. Early detection and classification of the lesion improve the prognosis and assist in early direct treatment consisting of surgical exposure and removal of granulation tissue from the resorbing lacunae and sealing.
Replacement external resorption associated with root canal filled right maxillary central incisor. An oblique multiplanar reformatted “panoramic” image (a) shows the dentition with minimal restorations and a single root canal filled maxillary right central incisor; note that the obturation is large in relation to the width of the adjacent left maxillary central suggesting endodontic treatment at an early age. Sequential 1 mm cross-sectional (b) and parasagittal (c) images show bone trabecular-like replacement of the superior and palatal aspects of the root indicative of replacement resorption. Initial management consisted of conventional endodontic treatment. Because of the questionable long-term prognosis of the apical resorptive lesions, periodic CBCT imaging is recommended with a view towards surgical revision therapy consisting of apicoectomy and retrograde root canal treatment (data acquired on an iCAT, Imaging Sciences International, Hatfield, PA USA at 0.4 mm resolution and reformatted using InVivo Dental, Anatomage, San Jose, CA).
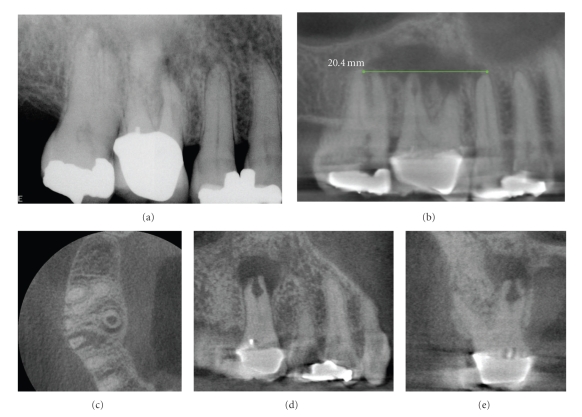
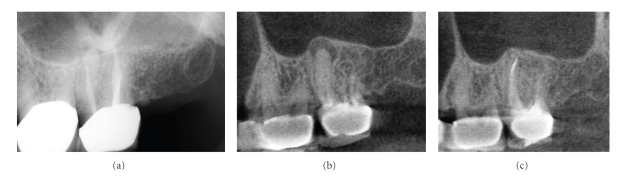
Because two-dimensional imaging suffers from superimposition of anatomic structures, determination of the extent and pathogenesis of periradicular lesions can present diagnostic challenges. This is particularly true of the maxillary posterior region, where the roots of teeth overlap and anatomic structures form complex patterns. A patient presented with discomfort in the maxillary right that extended from the nose to the ear. On clinical examination buccal swelling and induration were present—all teeth tested vital except the maxillary right first molar. A periapical radiograph (a) demonstrated areas of low density at the apices of the maxillary right first and second molars. CBCT images ((b) 10 mm curved planar, (c) axial, (d) sagittal, (e) cross-sectional) however demonstrated a much more extensive (21.4 mm maximum length) unilocular lesion, centered on the palatal root of the maxillary first molar, and extending anteriorly to the second bicuspid and posteriorly to the second molar. Also note the large internal resorptive lesion at the mid-palatal root of the maxillary first molar, not visible on the periapical radiograph. Biopsy confirmed the lesion to be a periapical granuloma with abscess formation.
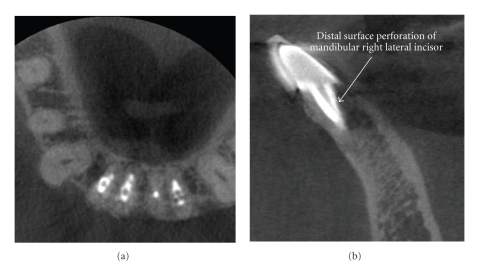
Iatrogenic perforative defects can be difficult to confirm by periapical radiography alone. This patient was referred for evaluation and possible endodontic revision of the mandibular right lateral incisor because of chronic sensitivity to occlusal forces. CBCT images ((a) axial, (b) sagittal) demonstrate a mid-root post perforation.
References
-
- Langland OE, Langlais RP. Early pioneers of oral and maxillofacial radiology. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 1995;80(5):496–511. - PubMed
-
- Jacobsohn PH, Fedran RJ. Making darkness visible: the discovery of X-ray and its introduction to dentistry. The Journal of the American Dental Association. 1995;126(10):1359–1367. - PubMed
-
- Farman AG, Levato CM, Scarfe WC. 3D X-ray: an update. Inside Dentistry. 2007;3(6):70–74.
-
- Walton RE. Diagnostic imaging A. endodontic radiography. In: Ingle JI, Bakland LK, Baumgartner JC, editors. Ingles’ Endodontics. 6th edition. Hamilton, Canada: BC Decker; 2008. p. 554.
-
- Rushton VE, Horner K, Worthington HV. Screening panoramic radiology of adults in general dental practice: radiological findings. British Dental Journal. 2001;190(9):495–501. - PubMed
LinkOut - more resources
Full Text Sources
