

Diagnostic accuracy of 64-slice computed tomography coronary angiography for the detection of in-stent restenosis: a meta-analysis
- PMID: 20379863
- PMCID: PMC2866963
- DOI: 10.1007/s12350-010-9218-2
Diagnostic accuracy of 64-slice computed tomography coronary angiography for the detection of in-stent restenosis: a meta-analysis
Abstract
Background: We sought to evaluate the diagnostic accuracy of 64-slice multi-detector row computed tomography (MDCT) compared with invasive coronary angiography for in-stent restenosis (ISR) detection.
Methods: MEDLINE, Cochrane library, and BioMed Central database searches were performed until April 2009 for original articles. Inclusion criteria were (1) 64-MDCT was used as a diagnostic test for ISR, with >50% diameter stenosis selected as the cut-off criterion for significant ISR, using invasive coronary angiography and quantitative coronary angiography as the standard of reference; (2) absolute numbers of true positive, false positive, true negative, and false negative results could be derived. Standard meta-analytic methods were applied.
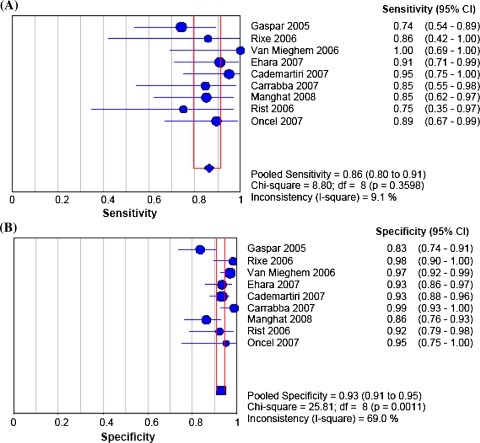
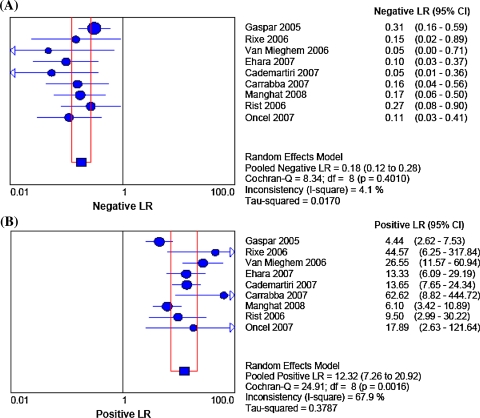
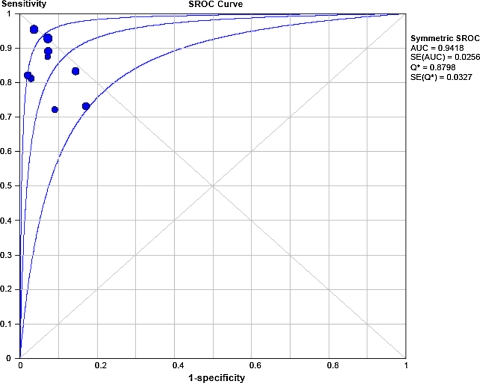
Results: Nine studies with a total of 598 patients with 978 stents included were considered eligible. On average, 9% of stents were unassessable (range 0-42%). Accuracy tests with 95% confidence intervals (CIs) comparing 64-MDCT vs invasive coronary angiography showed that pooled sensitivity, specificity, positive and negative likelihood ratio (random effect model) values were: 86% (95% CI 80-91%), 93% (95% CI 91-95%), 12.32 (95% CI 7.26-20.92), 0.18 (95% CI 0.12-0.28) for binary ISR detection. The symmetric area under the curve value was 0.94, indicating good agreement between 64-MDCT and invasive coronary angiography.
Conclusions: 64-MDCT has a good diagnostic accuracy for ISR detection with a particularly high negative predictive value. However, still a relatively large proportion of stents remains uninterpretable. Accordingly, only in selected patients, 64-MDCT may serve as a potential alternative noninvasive method to rule out ISR.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
