

A systematic review of the impact of sedation practice in the ICU on resource use, costs and patient safety
- PMID: 20380720
- PMCID: PMC2887180
- DOI: 10.1186/cc8956
A systematic review of the impact of sedation practice in the ICU on resource use, costs and patient safety
Abstract
Introduction: Patients in intensive care units (ICUs) often receive sedation for prolonged periods. In order to better understand the impact of sub-optimal sedation practice on outcomes, we performed a systematic review, including observational studies and controlled trials which were conducted in sedated patients in the ICU and which compared the impact of changes in or different protocols for sedation management on economic and patient safety outcomes.
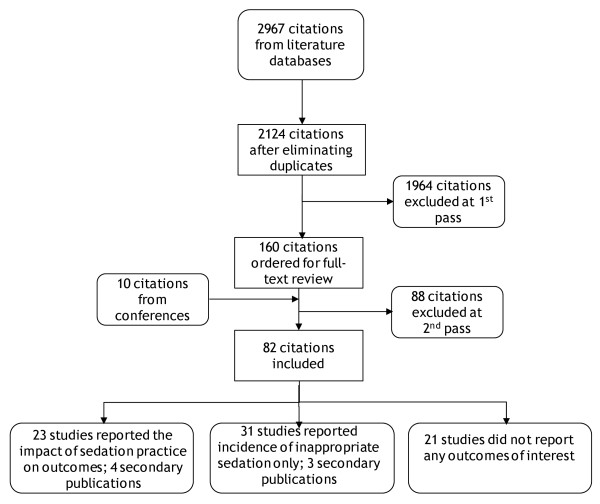
Methods: We searched Medline, Embase and CINAHL online literature databases from 1988 to 15th May 2008 and hand searched conferences. English-language studies set in the ICU, in sedated adult humans on mechanical ventilation, which reported the impact of sedation practice on cost and resource use and patient safety outcomes, were included. All abstracts were reviewed twice by two independent reviewers, with all conflicts resolved by a third reviewer, to check that they met the review inclusion criteria. Full-text papers of all included studies were retrieved and again reviewed twice against inclusion criteria. Data were doubly extracted from studies. Study aims, design, population, and outcomes including duration of mechanical ventilation, length of stay in ICU and hospital, costs and rates of mortality and adverse events were extracted. Due to heterogeneity between study designs and outcomes reported, no quantitative data synthesis such as meta-analysis was possible.
Results: Included studies varied in design, patient population and aim, with the majority being before-after studies. Overall, studies showed that improvements in sedation practice, such as the introduction of guidelines and protocols, or daily interruption of sedation, were associated with improvements in outcomes including ICU and hospital length of stay, duration of mechanical ventilation, and costs. Mortality and the incidence of nosocomial infections were also reduced.
Conclusions: Systematic interventions to improve sedation practice and maintain patients at an optimal sedation level in the ICU may improve patient outcomes and optimize resource usage.
Figures
Comment in
-
Liberation and animation for ventilated ICU patients: the ABCDE bundle for the back-end of critical care.Crit Care. 2010;14(3):157. doi: 10.1186/cc8999. Epub 2010 May 20. Crit Care. 2010. PMID: 20497606 Free PMC article.
References
-
- SIGN. Methodology - search filters [Report] http://www.sign.ac.uk/methodology/filters.html
-
- Costa J, Cabre L, Molina R, Carrasco G. Cost of ICU sedation: comparison of empirical and controlled sedation methods. Clin Intensive Care. 1994;5:17–21. - PubMed
-
- Burns SM, Earven S, Fisher C, Lewis R, Merrell P, Schubart JR, Truwit JD, Bleck TP. University of Virginia Long Term Mechanical Ventilation Team. Implementation of an institutional program to improve clinical and financial outcomes of mechanically ventilated patients: one-year outcomes and lessons learned[see comment] Crit Care Med. 2003;31:2752–2763. doi: 10.1097/01.CCM.0000094217.07170.75. - DOI - PubMed
-
- Kress JP, Pohlman AS, Hall JB. Effects of sedative interruption in critically ill, mechanically ventilated patients receiving midazolam or propofol. JCOM. 2001;8:33–39.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
