

Congenital idiopathic hypogonadotropic hypogonadism: evidence of defects in the hypothalamus, pituitary, and testes
- PMID: 20382682
- PMCID: PMC2902061
- DOI: 10.1210/jc.2009-2582
Congenital idiopathic hypogonadotropic hypogonadism: evidence of defects in the hypothalamus, pituitary, and testes
Abstract
Context: Idiopathic hypogonadotropic hypogonadism (IHH) with normal smell (normosmic IHH) or anosmia (Kallmann syndrome) is associated with defects in the production or action of GnRH. Accordingly, most IHH patients respond to physiological pulsatile GnRH replacement by normalizing serum LH, FSH, and testosterone (T) levels and achieving gametogenesis; some patients, however, show atypical responses. Interestingly, several IHH-associated genes are expressed in multiple compartments of the hypothalamic-pituitary-gonadal axis.
Objective: The aim of the study was to investigate whether the clinical, biochemical, or genetic characteristics of IHH men with atypical responses to GnRH indicate alternative or additional defects in the hypothalamic-pituitary-gonadal axis.
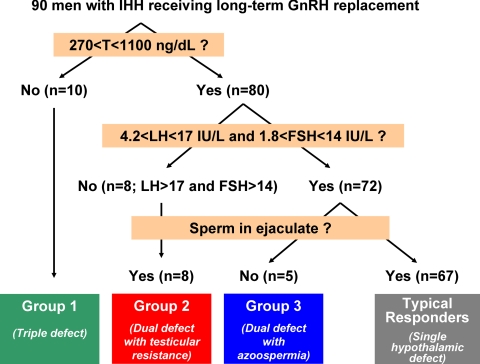
Subjects: We studied 90 IHH men undergoing long-term pulsatile GnRH treatment over 30 yr.
Design and setting: We conducted a retrospective study of response to GnRH at a Clinical Research Center.
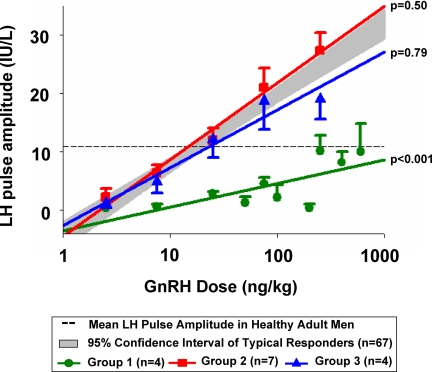
Interventions: Physiological regimens of pulsatile s.c. GnRH were administered for at least 12 months. Dose-response studies using i.v. GnRH pulses assessed the pituitary LH response.
Main outcome measures: We measured serum T, LH, FSH, and inhibin B levels, sperm in ejaculate, and determined the sequence of IHH-associated genes.
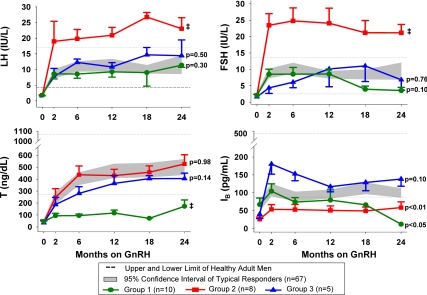
Results: Twenty-six percent of subjects displayed atypical responses to GnRH: 1) 10 remained hypogonadotropic and hypogonadal, demonstrating pituitary and testicular defects; 2) eight achieved spermatogenesis and normal T but only with hypergonadotropism, indicating impaired testicular responsiveness to gonadotropins; and 3) five remained azoospermic despite achieving adult testicular volumes and normal hormonal profiles, suggesting primary defects in spermatogenesis. Mutations were identified only in KAL1 across groups.
Conclusion: In addition to hypothalamic GnRH deficiency, IHH men can have primary pituitary and/or testicular defects, which are unmasked by GnRH replacement.
Figures
Similar articles
-
Responsiveness to a physiological regimen of GnRH therapy and relation to genotype in women with isolated hypogonadotropic hypogonadism.J Clin Endocrinol Metab. 2013 Feb;98(2):E206-16. doi: 10.1210/jc.2012-3294. Epub 2013 Jan 22. J Clin Endocrinol Metab. 2013. PMID: 23341491 Free PMC article. Clinical Trial.
-
Predictors of outcome of long-term GnRH therapy in men with idiopathic hypogonadotropic hypogonadism.J Clin Endocrinol Metab. 2002 Sep;87(9):4128-36. doi: 10.1210/jc.2002-020518. J Clin Endocrinol Metab. 2002. PMID: 12213860 Clinical Trial.
-
Predictive factors for pituitary response to pulsatile GnRH therapy in patients with congenital hypogonadotropic hypogonadism.Asian J Androl. 2018 Jul-Aug;20(4):319-323. doi: 10.4103/aja.aja_83_17. Asian J Androl. 2018. PMID: 29516878 Free PMC article.
-
[Clinical and molecular aspects of congenital isolated hypogonadotropic hypogonadism].Arq Bras Endocrinol Metabol. 2011 Nov;55(8):501-11. doi: 10.1590/s0004-27302011000800002. Arq Bras Endocrinol Metabol. 2011. PMID: 22218430 Review. Portuguese.
-
Molecular genetics of isolated hypogonadotropic hypogonadism and Kallmann syndrome.Endocr Dev. 2005;8:67-80. doi: 10.1159/000084094. Endocr Dev. 2005. PMID: 15722618 Review.
Cited by
-
Conditional Fgfr1 Deletion in GnRH Neurons Leads to Minor Disruptions in the Reproductive Axis of Male and Female Mice.Front Endocrinol (Lausanne). 2021 Feb 19;11:588459. doi: 10.3389/fendo.2020.588459. eCollection 2020. Front Endocrinol (Lausanne). 2021. PMID: 33679600 Free PMC article.
-
Efficacy and Outcome Predictors of Gonadotropin Treatment for Male Congenital Hypogonadotropic Hypogonadism: A Retrospective Study of 223 Patients.Medicine (Baltimore). 2016 Mar;95(9):e2867. doi: 10.1097/MD.0000000000002867. Medicine (Baltimore). 2016. PMID: 26945370 Free PMC article.
-
Responsiveness to a physiological regimen of GnRH therapy and relation to genotype in women with isolated hypogonadotropic hypogonadism.J Clin Endocrinol Metab. 2013 Feb;98(2):E206-16. doi: 10.1210/jc.2012-3294. Epub 2013 Jan 22. J Clin Endocrinol Metab. 2013. PMID: 23341491 Free PMC article. Clinical Trial.
-
Follicle-stimulating hormone signaling in Sertoli cells: a licence to the early stages of spermatogenesis.Reprod Biol Endocrinol. 2022 Jul 2;20(1):97. doi: 10.1186/s12958-022-00971-w. Reprod Biol Endocrinol. 2022. PMID: 35780146 Free PMC article. Review.
-
Gonadotropin-Induced Spermatogenesis in CHH Patients with Cryptorchidism.Int J Endocrinol. 2019 Dec 18;2019:6743489. doi: 10.1155/2019/6743489. eCollection 2019. Int J Endocrinol. 2019. PMID: 31929795 Free PMC article.
References
-
- Belchetz PE, Plant TM, Nakai Y, Keogh EJ, Knobil E 1978 Hypophysial responses to continuous and intermittent delivery of hypothalamic gonadotropin-releasing hormone. Science 202:631–633 - PubMed
-
- Hoffman AR, Crowley Jr WF 1982 Induction of puberty in men by long-term pulsatile administration of low-dose gonadotropin-releasing hormone. N Engl J Med 307:1237–1241 - PubMed
-
- Pitteloud N, Hayes FJ, Dwyer A, Boepple PA, Lee H, Crowley Jr WF 2002 Predictors of outcome of long-term GnRH therapy in men with idiopathic hypogonadotropic hypogonadism. J Clin Endocrinol Metab 87:4128–4136 - PubMed
-
- Waldstreicher J, Seminara SB, Jameson JL, Geyer A, Nachtigall LB, Boepple PA, Holmes LB, Crowley Jr WF 1996 The genetic and clinical heterogeneity of gonadotropin-releasing hormone deficiency in the human. J Clin Endocrinol Metab 81:4388–4395 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
