

Review
doi: 10.1007/s10456-010-9167-z.
Epub 2010 Apr 11.
Non-invasive imaging of angiogenesis in head and neck squamous cell carcinoma
Affiliations
- PMID: 20383743
- PMCID: PMC2912423
- DOI: 10.1007/s10456-010-9167-z
Item in Clipboard
Review
Non-invasive imaging of angiogenesis in head and neck squamous cell carcinoma
Angiogenesis.
2010 Jun.
Abstract
Squamous cell carcinoma of the head and neck (HNSCC) is the seventh most common cancer in the United States. Angiogenesis, the process by which new blood vessels are formed, is an essential element at the basis of both tumor growth and metastases. This review discusses pertinent aspects of the role of imaging modalities in assessing angiogenesis and anti-angiogenic therapy in advanced HNSCC.
Figures
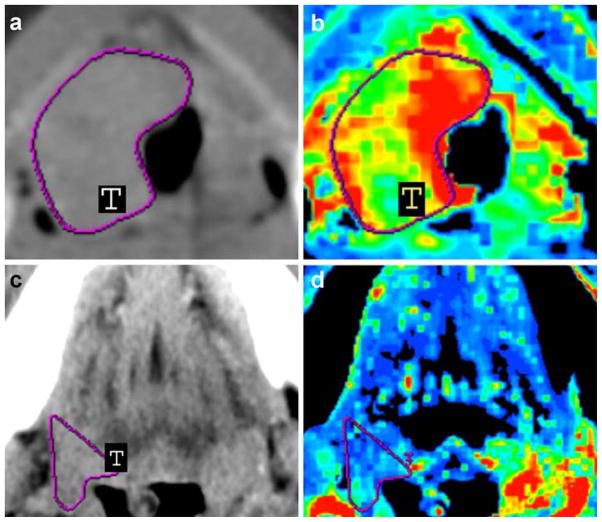
Contrast-enhanced neck CT scans (a, c) and CT perfusion maps (b, d) of a 45-year-old man with stage IV (a–b) and a 57-year-old woman with stage III (c–d) HNSCC in the base of the tongue. Solid tumor masses are indicated with T in (a, c). CT perfusion map (b) shows elevated blood flow (190.15 ml/100 g/min), which was confirmed by relative increased intratumoral MVD (47.2 vessels per square millimeter), whereas CT perfusion map (d) shows decreased blood flow (39.13 ml/100 g/min), which was confirmed by relative decreased intratumoral MVD (19.2 vessels per square millimeter). Reprinted with permission from [26]
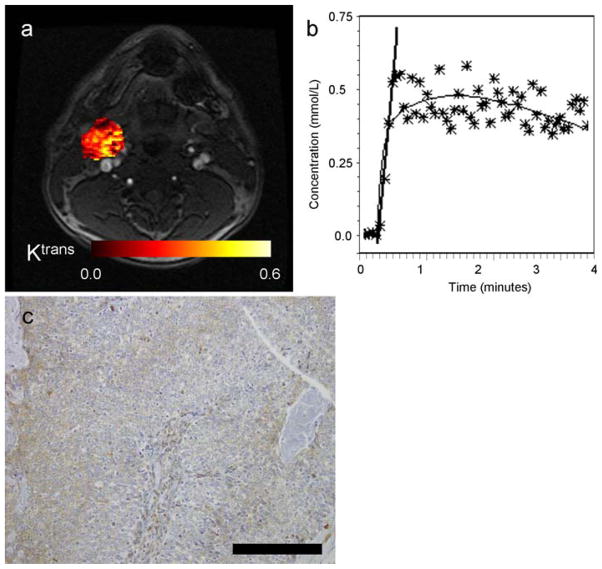
Images illustrating the left neck lymph node of a patient with HNSCC (male, 49 years old, primary cancer unknown). a Post-contrast axial MR image extracted from the DCE-MRI scan with the calculated parametric Ktrans map of the node overlaid on the DCE-MR image. b DCE-MRI signal, converted into Gd-DTPA concentrations, as a function of acquisition time. The stars indicate the individual data points (averaged over the ROI), the thin black line is the fit, and the thick black line indicates the slope. c VEGF immunostaining of corresponding tumor surgical specimen, indicating high expression. Black bar indicates 0.2 mm
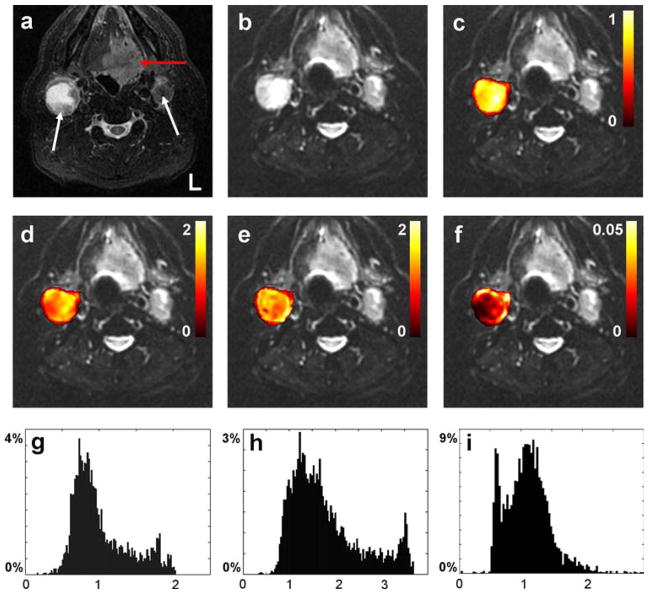
Axial MR images from the oral cavity of 60-year-old man diagnosed with HNSCC in the base of the tongue. a T2 short tau inversion recovery (STIR) image, b realigned mean b = 0 image. The red and white arrows in (a) indicate the primary tumor and metastatic nodes, respectively. Figures (c–f) display voxel-by-voxel calculation outcomes for the right node presented as mask overlays on the realigned mean b = 0 image. Graphs (g–i) display the corresponding histogram distribution plots of the measures from (c–e). c, g Apparent diffusion coefficient obtained from Gaussian monoexponential fitting (10−3 mm2/s). d, h Apparent diffusion coefficient (10−3 mm2/s), e, i apparent kurtosis coefficient (dimensionless), and f reduced χ2 error estimate, all obtained from the non-Gaussian diffusional kurtosis analysis. Reprinted with permission from [41]
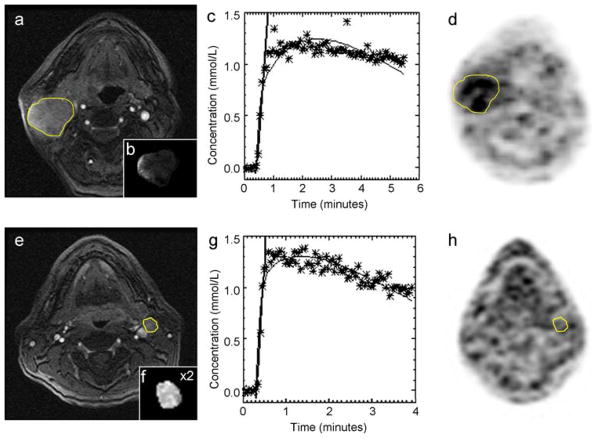
a–d MRI and 18F-FMISO PET images illustrating the hypoxic right neck lymph node of a patient (male, 62 years old, primary tonsil cancer). a Shows the post-contrast multi-phase spoiled gradient echo. The node is outlined in yellow. The insert (b) in (a) displays the calculated parametric Ktrans map of the node. In (c), the DCE-MRI signal (converted into Gd-DTPA concentrations) over the acquisition time is illustrated. The stars indicate the individual data points (averaged over the ROI), the thin black line is the fit, and the thick black line indicates the slope. Finally, in (d) the corresponding 18F-FMISO image is shown, indicating 18F-FMISO uptake in the node outlined in yellow. (e–h) MRI and 18F-FMISO PET images illustrating the non-hypoxic left neck lymph node of a patient (male, 51 years old, primary tonsil cancer). Reprinted with permission from [62]
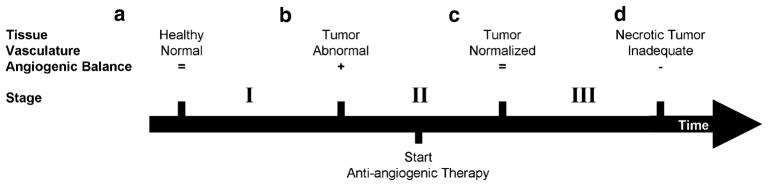
Schematic of changes in tumor vasculature during tumor formation and the course of anti-angiogenic therapy. a Healthy tissue has normal vasculature, which is composed of mature vessels and has an exact balance of pro- and anti-angiogenic molecules. b The activation of the angiogenic switch enables the tumor to engage surrounding blood vessels and promote formation of new vessels. The abnormal tumor vasculature provides the tumor with oxygen and nutrients, which facilitate more growth. c Administration of anti-angiogenic therapies prune immature vessels, which results in more normalized tumor vasculature (as proposed by Jain [84]). The resulting network is more effective for the transport of therapeutics and nutrients. d Rapid pruning of tumor vasculature reduces the integrity of vasculature network. The network is unable to facilitate tumor growth and could result in tumor dormancy, which is the ultimate goal of anti-angiogenic therapy. Figure conceptualized from [79] and [85]. Table 1 shows angiogenesis-related processes during the stages of tumor formation (I) and eradication (II–III), and best suited imaging modalities for their assessment
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics. CA Cancer J Clin. 2009;59:225–249. - PubMed
-
- Vokes EE, Weichselbaum RR, Lippman SM, Hong WK. Head and neck cancer. N Engl J Med. 1993;328:184–194. - PubMed
-
- Klem ML, Mechalakos JG, Wolden SL, Zelefsky MJ, Singh B, Kraus D, Shaha A, Shah J, Pfister DG, Lee NY. Intensity-modulated radiotherapy for head and neck cancer of unknown primary: toxicity and preliminary efficacy. Int J Radiat Oncol Biol Phys. 2008;70:1100–1107. - PubMed
-
- Lee NY, O’Meara W, Chan K, Della-Bianca C, Mechalakos JG, Zhung J, Wolden SL, Narayana A, Kraus D, Shah JP, Pfister DG. Concurrent chemotherapy and intensity-modulated radiotherapy for locoregionally advanced laryngeal and hypo-pharyngeal cancers. Int J Radiat Oncol Biol Phys. 2007;69:459–468. - PubMed
-
- Schwartz LH, Ozsahin M, Zhang GN, Touboul E, De Vataire F, Andolenko P, Lacau-Saint-Guily J, Laugier A, Schlienger M. Synchronous and metachronous head and neck carcinomas. Cancer. 1994;74:1933–1938. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
