

Use of a conventional low neck field (LNF) and intensity-modulated radiotherapy (IMRT): no clinical detriment of IMRT to an anterior LNF during the treatment of head-and neck-cancer
- PMID: 20385457
- PMCID: PMC3339153
- DOI: 10.1016/j.ijrobp.2009.10.034
Use of a conventional low neck field (LNF) and intensity-modulated radiotherapy (IMRT): no clinical detriment of IMRT to an anterior LNF during the treatment of head-and neck-cancer
Abstract
Purpose: To determine differences in clinical outcomes using intensity-modulated radiotherapy (IMRT) or a standard low neck field (LNF) to treat low neck.
Methods and materials: This is a retrospective, single-institution study. Ninety-one patients with squamous cell carcinoma of the head and neck were treated with curative intent. According to physician preference, some patients were treated with LNF (Planning Target Volume 3) field using a single anterior photon field matched to the IMRT field. Field junctions were not feathered. The endpoints were time to failure and use of a percutaneous endoscopic gastrostomy (PEG) tube (as a surrogate of laryngeal edema causing aspiration), and analysis was done with χ(2) and log-rank tests.
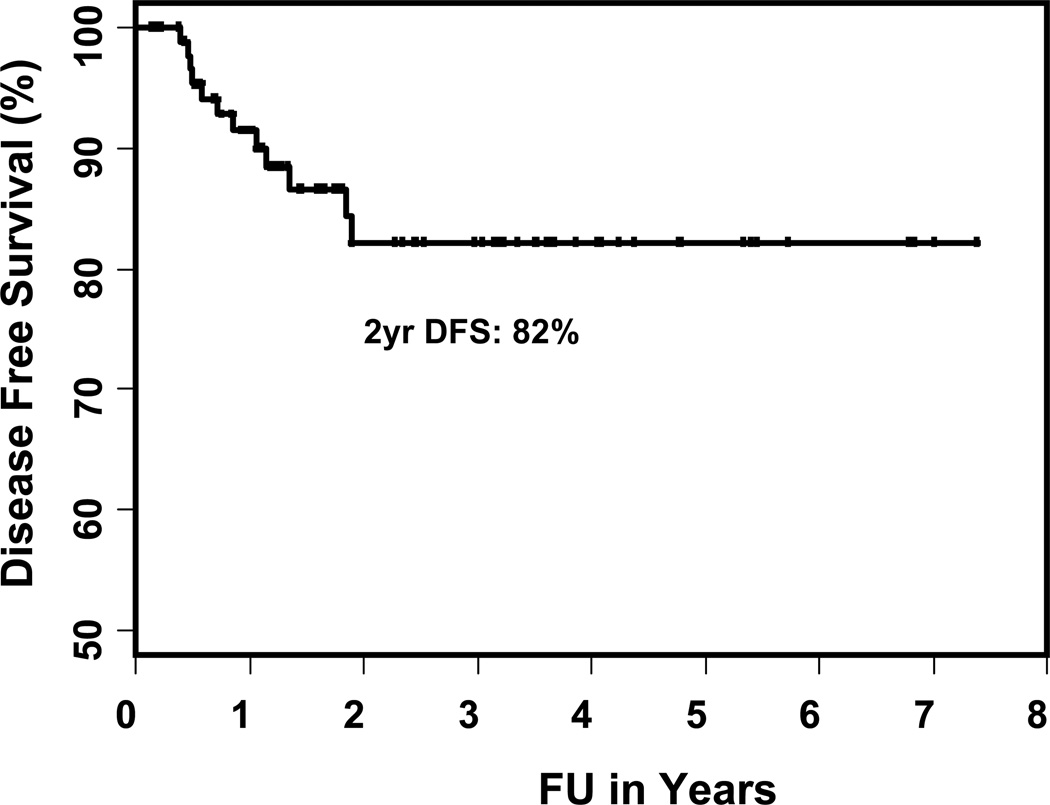
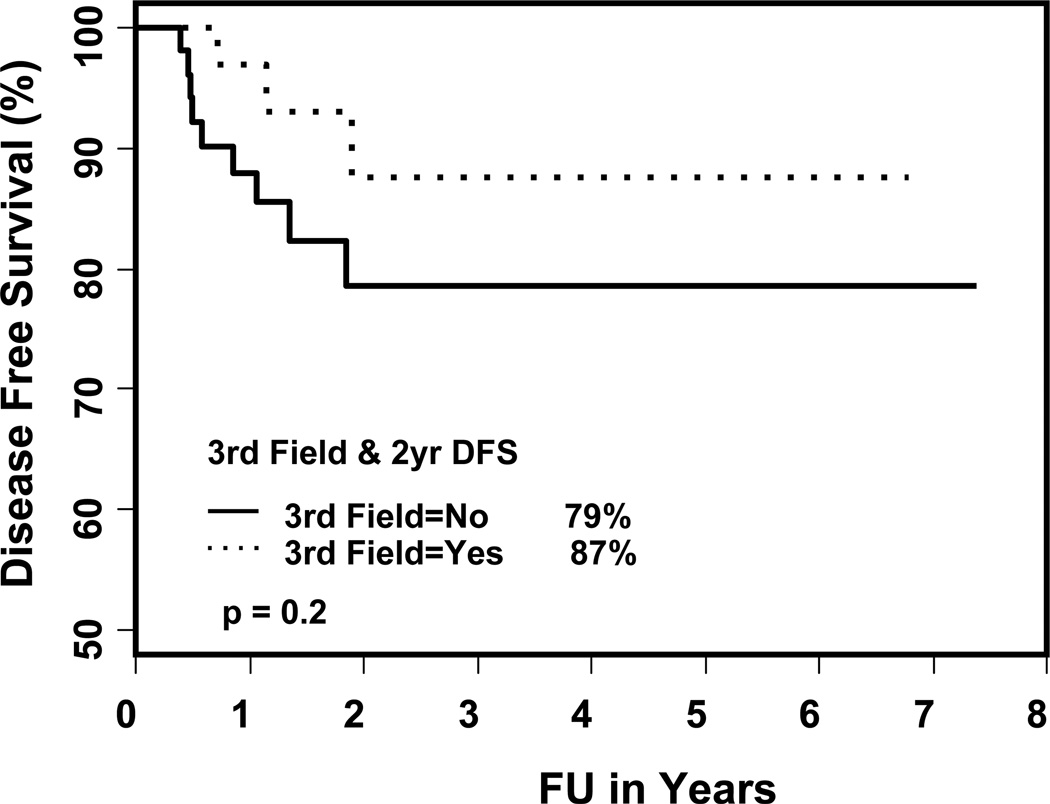
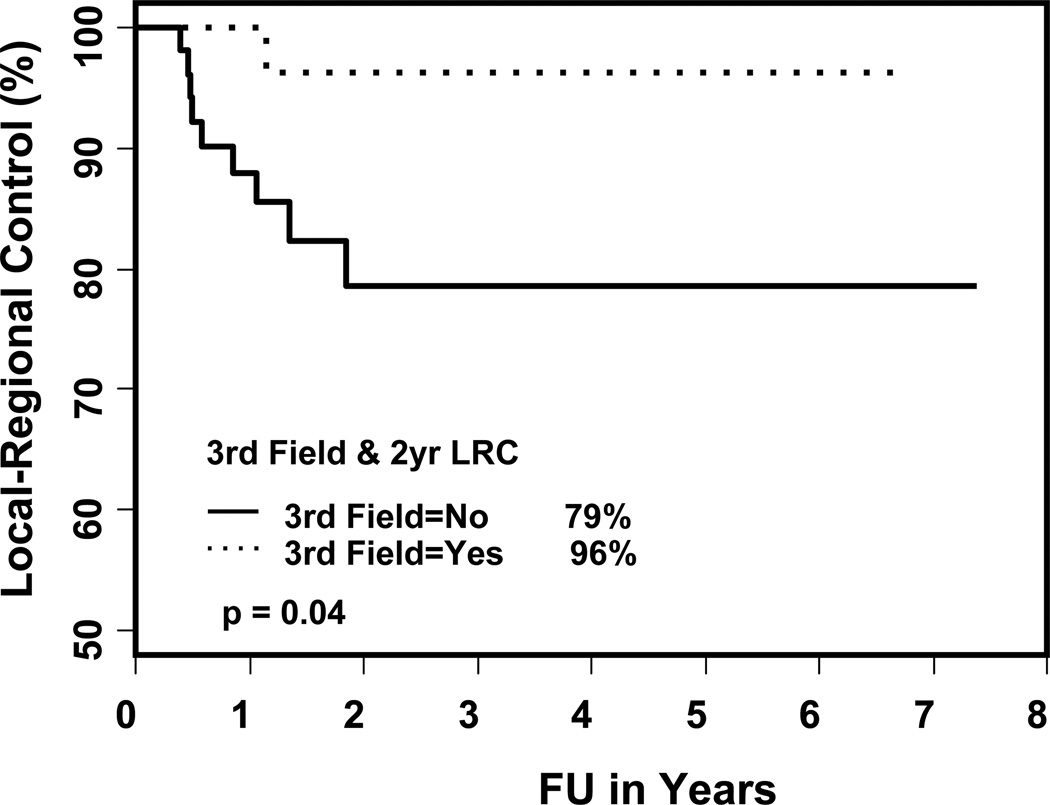
Results: Median follow-up was 21 months (range, 2-89 months). Median age was 60 years. Thirty-seven patients (41%) were treated with LNF, 84% were Stage III or IV. A PEG tube was required in 30%, as opposed to 33% without the use of LNF. Node 2 or 3 neck disease was treated more commonly without LNF (38% vs. 24%, p = 0.009). Failures occurred in 12 patients (13%). Only 1 patient treated with LNF failed regionally, 4.5 cm above the match line. The 3-year disease-free survival rate was 87% and 79% with LNF and without LNF, respectively (p = 0.2), and the 3-year LR failure rate was 4% and 21%, respectively (p = 0.04).
Conclusions: Using LNF to treat the low neck did not increase the risk of regional failure "in early T and early N diseases" or decrease PEG tube requirements.
Published by Elsevier Inc.
Figures
Similar articles
-
Regional relapse after intensity-modulated radiotherapy for head-and-neck cancer.Int J Radiat Oncol Biol Phys. 2011 Feb 1;79(2):450-8. doi: 10.1016/j.ijrobp.2009.10.028. Epub 2010 Apr 8. Int J Radiat Oncol Biol Phys. 2011. PMID: 20381266
-
Intensity-modulated radiotherapy for head and neck cancer of unknown primary: toxicity and preliminary efficacy.Int J Radiat Oncol Biol Phys. 2008 Mar 15;70(4):1100-7. doi: 10.1016/j.ijrobp.2007.07.2351. Epub 2007 Nov 5. Int J Radiat Oncol Biol Phys. 2008. PMID: 17980501
-
Intensity-modulated radiation treatment for head-and-neck squamous cell carcinoma--the University of Iowa experience.Int J Radiat Oncol Biol Phys. 2005 Oct 1;63(2):410-21. doi: 10.1016/j.ijrobp.2005.02.025. Int J Radiat Oncol Biol Phys. 2005. PMID: 16168834
-
Distant metastases in head-and-neck squamous cell carcinoma treated with intensity-modulated radiotherapy.Int J Radiat Oncol Biol Phys. 2012 Jun 1;83(2):684-9. doi: 10.1016/j.ijrobp.2011.07.014. Epub 2011 Dec 12. Int J Radiat Oncol Biol Phys. 2012. PMID: 22169673
-
Cervical lymph node metastases from unknown primary cancer: a single-institution experience with intensity-modulated radiotherapy.Int J Radiat Oncol Biol Phys. 2012 Apr 1;82(5):1866-71. doi: 10.1016/j.ijrobp.2011.02.031. Epub 2011 Apr 15. Int J Radiat Oncol Biol Phys. 2012. PMID: 21497452
Cited by
-
Effects of full-neck volumetric-modulated arc therapy vs split-field intensity-modulated head and neck radiation therapy on low neck targets and structures.Br J Radiol. 2016 Jun;89(1062):20160009. doi: 10.1259/bjr.20160009. Epub 2016 Apr 4. Br J Radiol. 2016. PMID: 27043353 Free PMC article.
References
-
- Eisbruch A, Ship JA, Dawson LA, et al. Salivary gland sparing and improved target irradiation by conformal and intensity modulated irradiation of head and neck cancer. World J Surg. 2003;27:832–837. - PubMed
-
- Chao KS, Ozyigit G, Tran BN, et al. Patterns of failure in patients receiving definitive and postoperative IMRT for head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2003;55:312–321. - PubMed
-
- Lee N, Xia P, Fischbein NJ, et al. Intensity-modulated radiation therapy for headand- neck cancer: the UCSF experience focusing on target volume delineation. Int J Radiat Oncol Biol Phys. 2003;57:49–60. - PubMed
-
- Eisbruch A, Marsh LH, Dawson LA, et al. Recurrences near base of skull after IMRT for head-and-neck cancer: implications for target delineation in high neck and for parotid gland sparing. Int J Radiat Oncol Biol Phys. 2004;59:28–42. - PubMed
-
- Schoenfeld GO, Amdur RJ, Morris CG, et al. Patterns of failure and toxicity after intensity-modulated radiotherapy for head and neck cancer. Int J Radiat Oncol Biol Phys. 2008;71:377–385. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
