

Granuloma encapsulation is a key factor for containing tuberculosis infection in minipigs
- PMID: 20386605
- PMCID: PMC2850319
- DOI: 10.1371/journal.pone.0010030
Granuloma encapsulation is a key factor for containing tuberculosis infection in minipigs
Abstract
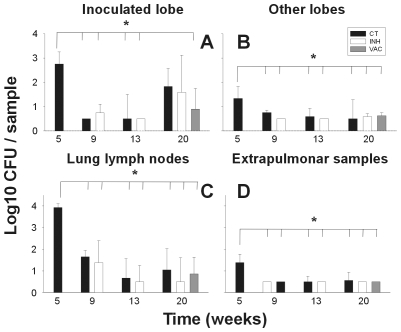
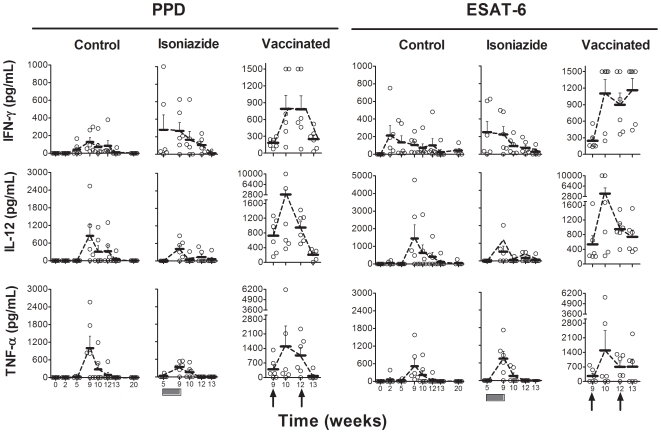
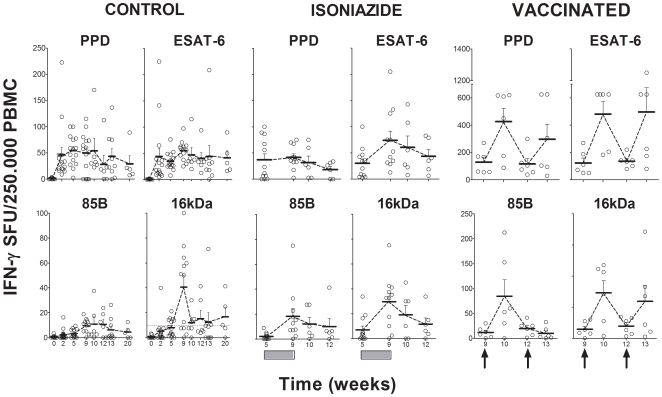
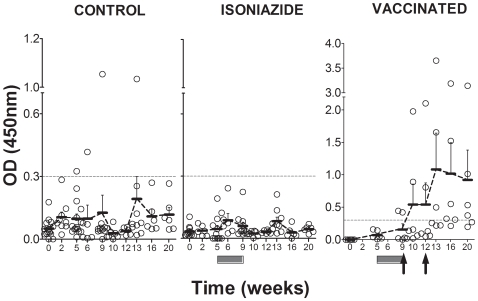
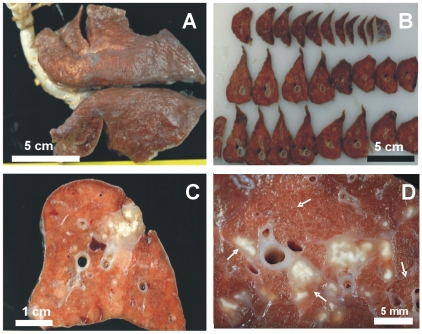
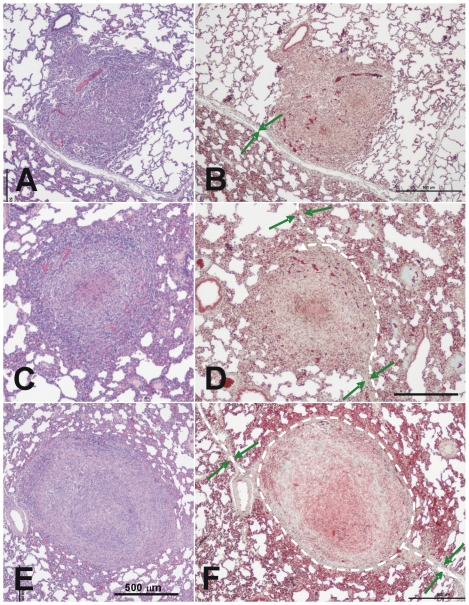
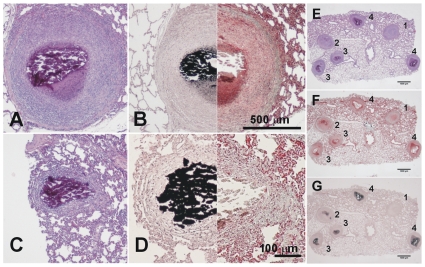
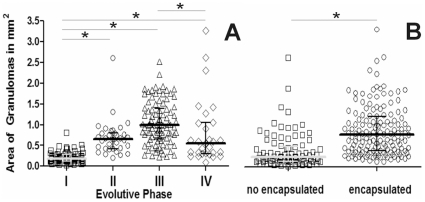
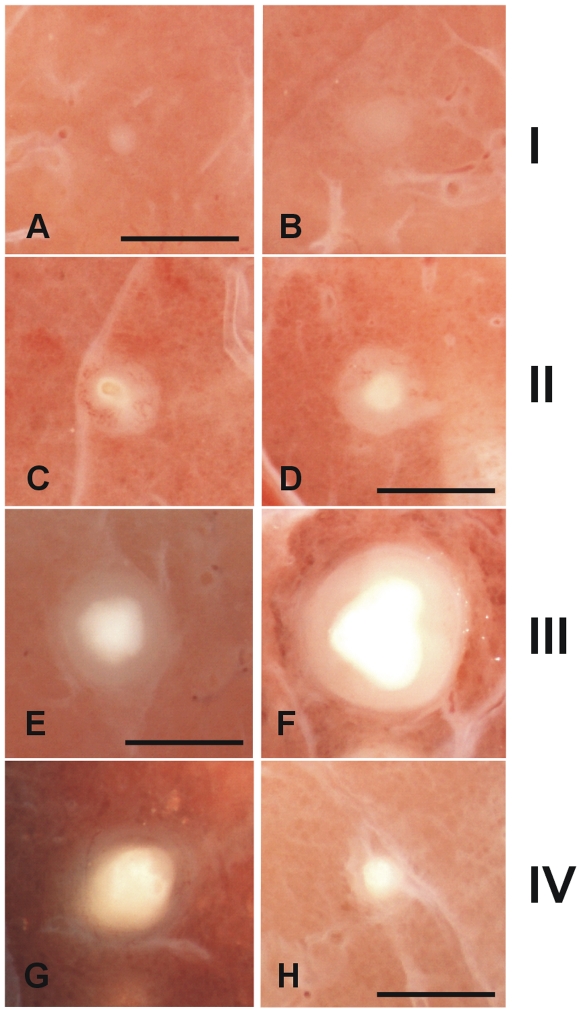
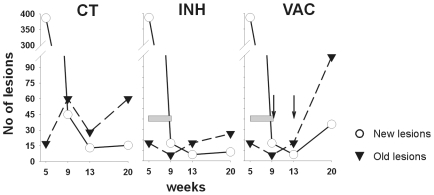
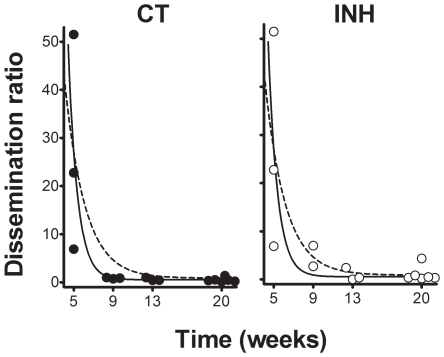
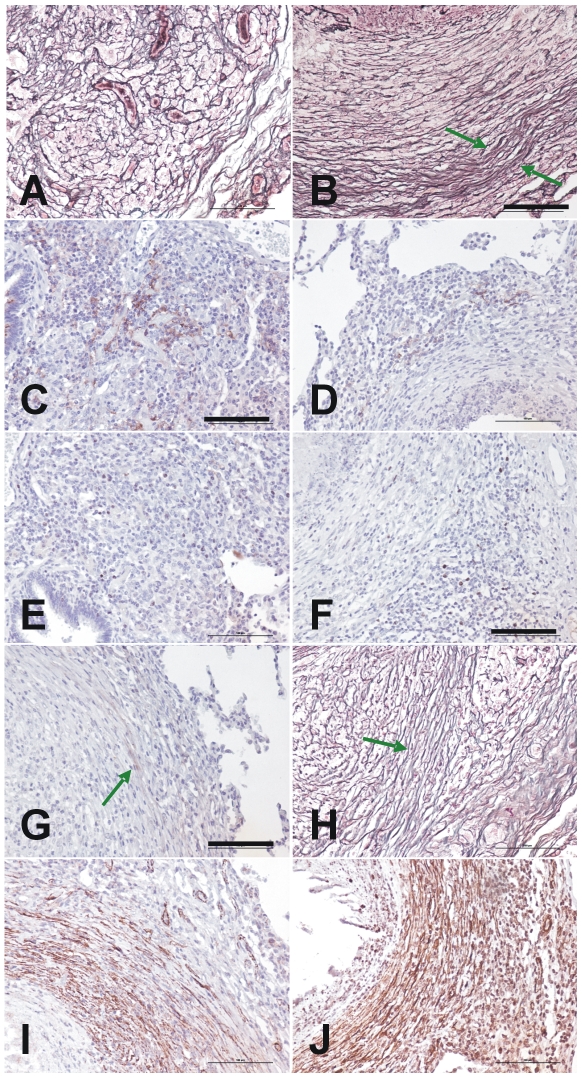
A transthoracic infection involving a low dose of Mycobacterium tuberculosis has been used to establish a new model of infection in minipigs. The 20-week monitoring period showed a marked Th1 response and poor humoral response for the whole infection. A detailed histopathological analysis was performed after slicing the formalin-fixed whole lungs of each animal. All lesions were recorded and classified according to their microscopic aspect, their relationship with the intralobular connective network and their degree of maturity in order to obtain a dissemination ratio (DR) between recent and old lesions. CFU counts and evolution of the DR with time showed that the proposed model correlated with a contained infection, decreasing from week 9 onwards. These findings suggest that the infection induces an initial Th1 response, which is followed by local fibrosis and encapsulation of the granulomas, thereby decreasing the onset of new lesions. Two therapeutic strategies were applied in order to understand how they could influence the model. Thus, chemotherapy with isoniazid alone helped to decrease the total number of lesions, despite the increase in DR after week 9, with similar kinetics to those of the control group, whereas addition of a therapeutic M. tuberculosis fragment-based vaccine after chemotherapy increased the Th1 and humoral responses, as well as the number of lesions, but decreased the DR. By providing a local pulmonary structure similar to that in humans, the mini-pig model highlights new aspects that could be key to a better understanding tuberculosis infection control in humans.
Conflict of interest statement
Figures
References
-
- WHO. Global tuberculosis control: epidemiology, strategy, financing: WHO report 2009. 2009. Geneva, Switzerland.
-
- Parrish N, Dick J, Bishai W. Mechanisms of latency in Mycobacterium tuberculosis. Trends Microbiol. 1998;6:107–112. - PubMed
-
- Sterling TR, Bethel J, Goldberg S, Weinfurter P, Yun L, et al. The scope and impact of treatment of latent tuberculosis infection in the United States and Canada. Am J Respir Crit Care Med. 2006;173:927–931. - PubMed
-
- Bucher HC, Griffith LE, Guyatt GH, Sudre P, Naef M, et al. Isoniazid prophylaxis for tuberculosis in HIV infection: a meta-analysis of randomized controlled trials. Aids. 1999;13:501–507. - PubMed
-
- Targeted tuberculin testing and treatment of latent tuberculosis infection. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. This is a Joint Statement of the American Thoracic Society (ATS) and the Centers for Disease Control and Prevention (CDC). This statement was endorsed by the Council of the Infectious Diseases Society of America. (IDSA), September 1999, and the sections of this statement. Am J Respir Crit Care Med. 2000;161:S221–247. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
