

Neoadjuvant sequential epirubicin and docetaxel followed by surgery-radiotherapy and post-operative docetaxel or gemcitabine/vinorelbine combination based on primary response: a multimodality approach for locally advanced breast cancer
- PMID: 20387073
- PMCID: PMC11828130
- DOI: 10.1007/s00432-010-0878-8
Neoadjuvant sequential epirubicin and docetaxel followed by surgery-radiotherapy and post-operative docetaxel or gemcitabine/vinorelbine combination based on primary response: a multimodality approach for locally advanced breast cancer
Abstract
Background: Locally advanced breast cancer (LABC) remains a major clinical issue despite progress achieved in recent years. Herein, we present the mature results of a multimodality treatment program tailoring epirubicin (EPI), docetaxel (DOC) and gemcitabine-vinorelbine (GEV) peri-operatively in LABC.
Patients and methods: Stage III, Eastern Cooperative Oncology Group-Performance status ≤2 patients were eligible. A biopsy documentation had to be performed before the start of chemotherapy (CT). Treatment consisted of four EPI (100 mg/m(2), d1q2w) followed by three DOC (100 mg/m(2), d1q3w); surgery 3-4 weeks from CT completion, followed by radiation therapy (RT) and CT according to response; partial or complete (PR/CR):DOC, no change or progressive disease (NC/PD):GEV. Primary endpoints were: (a) response and conversion to operability/conservative surgery and (b) overall survival (OS) and time to recurrence (TTR).
Results: Fifty-six women, aged 32-75 (median 52 years), 24 IIIA and 32 IIIB were enrolled; 53 patients completed the entire program. Toxicity was acceptable and no treatment-related death was observed.
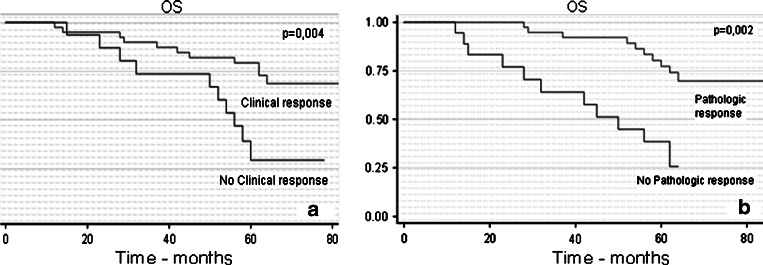
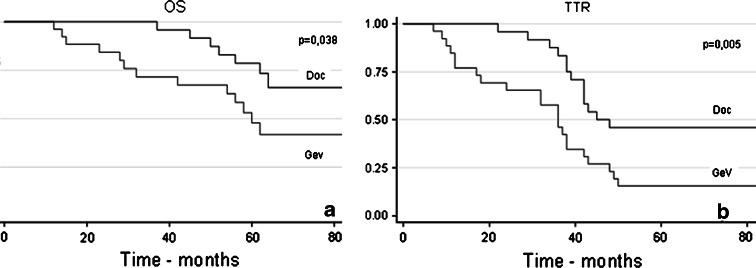
Efficacy: clinical response rate (RR) 71.4% (40 patients); clinical complete response rate 33.9% (19 patients). Pathological response rate (RR) 67.8% (38 patients); pathological complete response rate 21.4% (12 patients). 33 (58.9%) and 19 (33.9%) patients, respectively, had radical and conservative operations without increased morbidity. After a median follow-up of 62 months, median OS has not yet been reached, while median TTR was 42 months. OS was longer in patients with clinical (p = 0.004) and pathological response (p = 0.002), RT (p < 0.0001) and post-operative DOC (p = 0.038). TTR was favorably affected by pR (p < 0.0001), RT (p < 0.0004) and post-operative DOC (p = 0.005). Pre-operative CT seemed to be equally active throughout all subgroups according to histology, ER/PR and HER2 status.
Conclusion: The treatment program of the present study allowed for the completion of an effective therapy at the cost of acceptable toxicity. The results of this study suggest a central role of CT for LABC and the value of eventually dose-dense, EPI- and DOC-based CT in a large proportion of LABC patients, regardless of biological tumor profile. Furthermore, tumor response (cR, pR) is an important surrogate for patients survival and further therapy management.
Figures

References
-
- Ardavanis A, Scorilas A, Tryfonopoulos D et al (2006) Multidisciplinary therapy of locally far-advanced or inflammatory breast cancer with fixed perioperative sequence of epirubicin, vinorelbine, and Fluorouracil chemotherapy, surgery, and radiotherapy: long-term results. Oncologist 11(6):563–573 - PubMed
-
- Ardavanis A, Kountourakis P, Maliou S et al (2007) Gemcitabine and oral vinorelbine as salvage treatment in patients with advanced anthracycline- and taxane-pretreated breast cancer. Anticancer Res 27(4C):2989–2992 - PubMed
-
- Bear HD, Anderson S, Smith RE et al (2006) Sequential preoperative or postoperative docetaxel added to preoperative doxorubicin plus cyclophosphamide for operable breast cancer: national surgical adjuvant breast and bowel project protocol B-27. J Clin Oncol 24(13):2019–2027 - PubMed
-
- Bonnefoi H, Diebold-Berger S, Therasse P et al (2003) Locally advanced/inflammatory breast cancers treated with intensive epirubicin-based neoadjuvant chemotherapy: are there molecular markers in the primary tumour that predict for 5 year clinical outcome? Ann Oncol 14:406–413 - PubMed
-
- Buzdar AU, Valero V, Theriault RL et al (2003) Pathological complete response to chemotherapy is related to hormone receptor status [abstract]. In: 26th San Antonio Breast Cancer Symposium Abstr. 302. Breast Cancer Res Treat, vol 85, p 2
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
