

Current developments in salivary diagnostics
- PMID: 20387312
- PMCID: PMC2857781
- DOI: 10.2217/bmm.09.68
Current developments in salivary diagnostics
Abstract
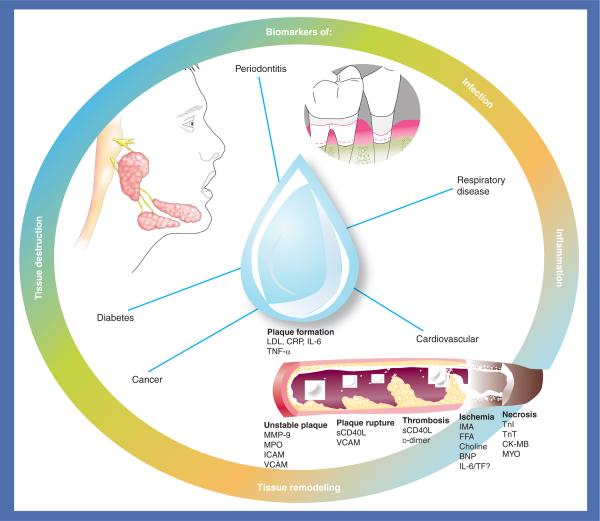
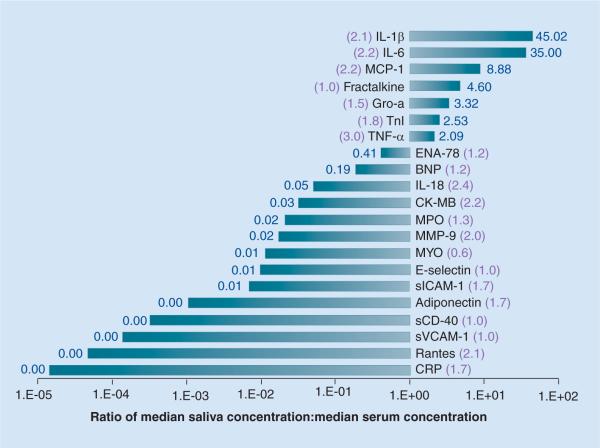
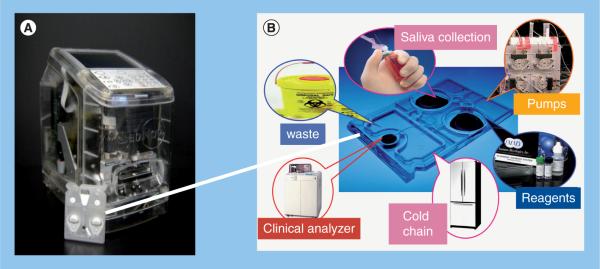
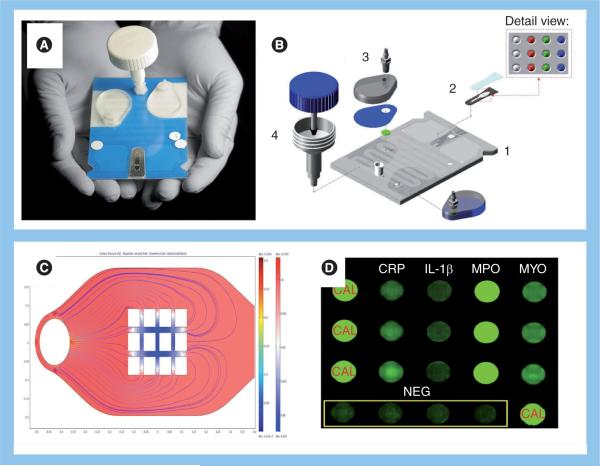
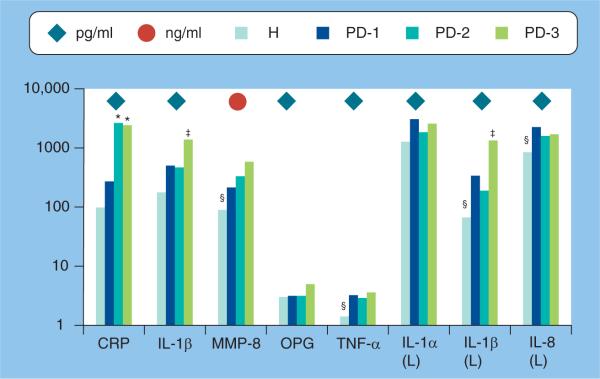
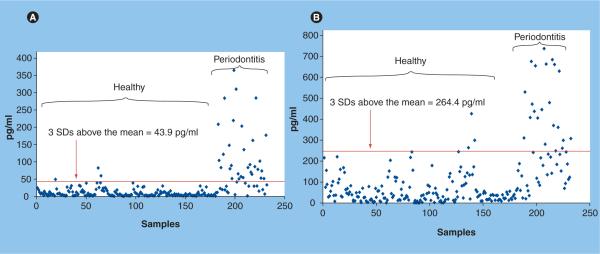
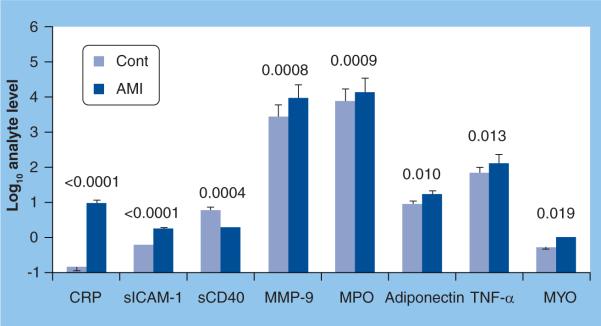
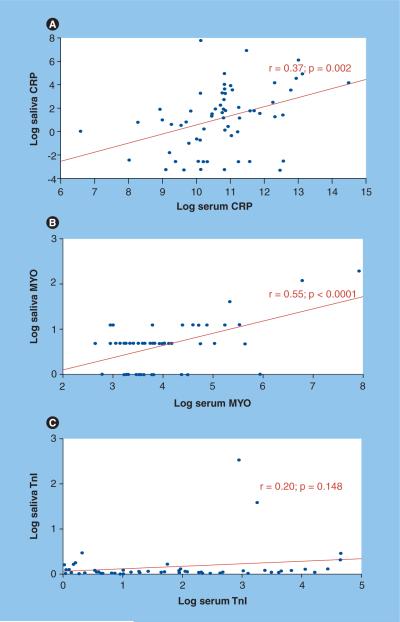
Salivary diagnostics is an emerging field that has progressed through several important developments in the past decade, including the publication of the human salivary proteome and the infusion of federal funds to integrate nanotechnologies and microfluidic engineering concepts into developing compact point-of-care devices for rapid analysis of this secretion. In this article, we discuss some of these developments and their relevance to the prognosis, diagnosis and management of periodontitis, as an oral target, and cardiovascular disease, as a systemic example for the potential of these biodiagnostics. Our findings suggest that several biomarkers are associated with distinct biological stages of these diseases and demonstrate promise as practical biomarkers in identifying and managing periodontal disease, and acute myocardial infarction. The majority of these studies have progressed through biomarker discovery, with the identified molecules requiring more robust clinical studies to enable substantive validation for disease diagnosis. It is predicted that with continued advances in this field the use of a combination of biomarkers in multiplex panels is likely to yield accurate screening tools for these diagnoses in the near future.
Figures
References
-
- Mandel ID. The diagnostic uses of saliva. J. Oral Pathol. Med. 1990;19(3):119–125. - PubMed
-
- Haeckel R, Hanecke P. The application of saliva, sweat and tear fluid for diagnostic purposes. Ann. Biol. Clin. (Paris) 1993;51(10–11):903–910. - PubMed
-
- Kaufman E, Lamster IB. The diagnostic applications of saliva — a review. Crit. Rev. Oral Biol. Med. 2002;13(2):197–212. - PubMed
-
- Malamud D, Niedbala RS, editors. Oral Based Diagnostics. Vol. 1098. Annals of the New York Academy of Sciences; Wiley-Blackwell, NY, USA: 2007. pp. 1–515. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous