

Delayed prehospital implementation of the 2005 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiac care
- PMID: 20388032
- PMCID: PMC3209500
- DOI: 10.3109/10903121003770639
Delayed prehospital implementation of the 2005 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiac care
Abstract
Introduction: In 2005, the American Heart Association (AHA) released guidelines to improve survival rates from out-of-hospital cardiac arrest (OHCA).
Objective: To determine if, and when, emergency medical services (EMS) agencies participating in the Resuscitation Outcomes Consortium (ROC) implemented these guidelines.
Methods: We contacted 178 EMS agencies and completed structured telephone interviews with 176 agencies. The survey collected data on specific treatment protocols before and after implementation of the 2005 guidelines as well as the date of implementation crossover (the "crossover date"). The crossover date was then linked to a database describing the size, type, and structure of each agency. Descriptive statistics and regression were used to examine patterns in time to crossover.
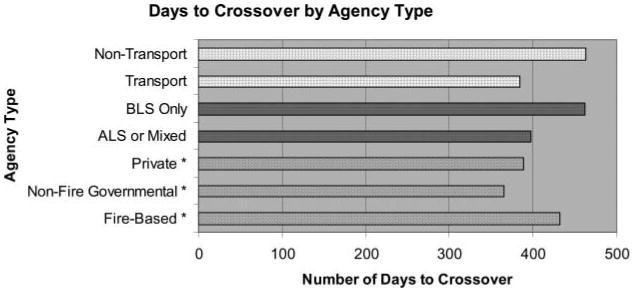
Results: The 2005 guidelines were implemented by 174 agencies (99%). The number of days from guideline release to implementation was as follows: mean 416 (standard deviation 172), median 415 (range 49-750). There was no difference in time to implementation in fire-based agencies (mean 432), nonfire municipal agencies (mean 365), and private agencies (mean 389, p = 0.31). Agencies not providing transport took longer to implement than agencies that transported patients (463 vs. 384 days, p = 0.004). Agencies providing only basic life support (BLS) care took longer to implement than agencies who provided advanced life support (ALS) care (mean 462 vs. 397 days, p = 0.03). Larger agencies (>10 vehicles) were able to implement the guidelines more quickly than smaller agencies (mean 386 vs. 442 days, p = 0.03). On average, it took 8.9 fewer days to implement the guidelines for every 50% increase in EMS-treated runs/year to which an agency responded.
Conclusion: ROC EMS agencies required an average of 416 days to implement the 2005 AHA guidelines for OHCA. Small EMS agencies, BLS-only agencies, and nontransport agencies took longer than large agencies, agencies providing ALS care, and transport agencies, respectively, to implement the guidelines. Causes of delays to guideline implementation and effective methods for rapid EMS knowledge translation deserve investigation.
Conflict of interest statement
None of the authors have any conflicts of interest, financial or otherwise, with regard to the article.
Figures



References
-
- Anonymous. American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2005;112(24 suppl):IV1–203. - PubMed
-
- Anonymous. American Heart Association Guidelines for CPR and ECC. Part 1. Introduction. Circulation. 2005;112(22 suppl):III-1–4.
-
- Anonymous. American Heart Association 2005 Guidelines for CPR and ECC. Part 3. Overview of CPR. Circulation. 2005;112(24 suppl):IV-12–8.
-
- Laerdal Foundation for Acute Medicine. [Accessed July 15, 2009];Utstein. Available at: http://www.laerdalfoundation.org/studier_hypoteser.html.
Publication types
MeSH terms
Grants and funding
- U01 HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077871/HL/NHLBI NIH HHS/United States
- HL077867/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- HL077873/HL/NHLBI NIH HHS/United States
- HL077871/HL/NHLBI NIH HHS/United States
- HL077881/HL/NHLBI NIH HHS/United States
- HL077908/HL/NHLBI NIH HHS/United States
- U01 HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- CAPMC/ CIHR/Canada
- U01 HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
- HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- HL077872/HL/NHLBI NIH HHS/United States
- HL077863/HL/NHLBI NIH HHS/United States
- HL077887/HL/NHLBI NIH HHS/United States
- 5U01/PHS HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- HL077885/HL/NHLBI NIH HHS/United States
- HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous