

G-CSF, rt-PA and combination therapy after experimental thromboembolic stroke
- PMID: 20388227
- PMCID: PMC2868804
- DOI: 10.1186/2040-7378-2-9
G-CSF, rt-PA and combination therapy after experimental thromboembolic stroke
Abstract
Background: Granulocyte Colony-Stimulating Factor (G-CSF) has remarkable neuroprotective properties. Due to its proven safety profile, G-CSF is currently used in clinical stroke trials. As neuroprotectants are considered to be more effective in the early phase of cerebral ischemia and during reperfusion, G-CSF should to be tested in combination with thrombolysis. Therefore, combination therapy was investigated in an experimental model of thromboembolic stroke.
Methods: Male Wistar rats (n = 72) were subjected to a model of thromboembolic occlusion (TE) of the middle cerebral artery. Different groups (n = 12 each) treated by recombinant tissue-plasminogen activator (rt-PA) or/and G-CSF: group control (control), group early G-CSF (G-CSF 60 min after TE), group rt-PA (rt-PA 60 min after TE), group com (combination rt-PA/G-CSF), group delayed rt-PA (rt-PA after 180 min), group deco (G-CSF after 60 min, rt-PA after 180 min). Animals were investigated by magnetic resonance imaging (MRI) and silver infarct staining (SIS) 24 hours after TE.
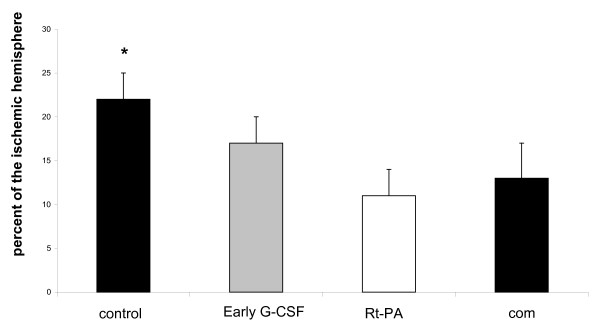
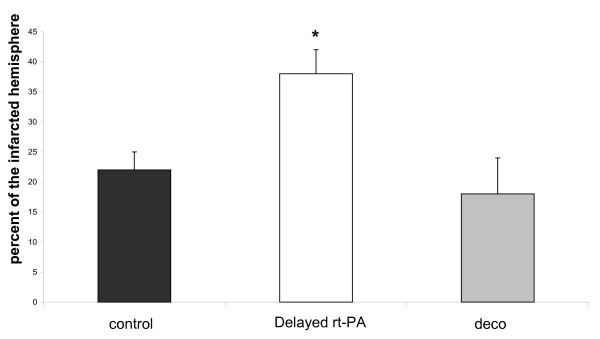
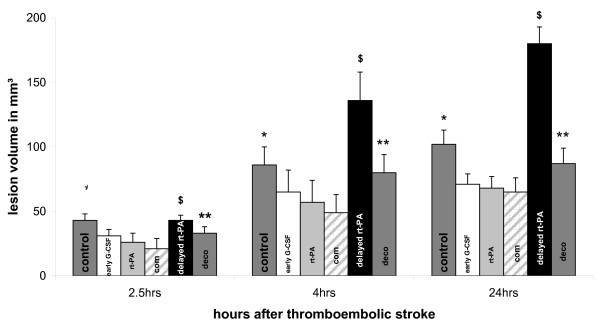
Results: Early G-CSF or rt-PA reduced the infarct size compared to all groups (p < 0.05 to p < 0.01) with the exception of group com, (p = n.s.) as measured by T2, DWI, and SIS. Late administration of rt-PA lead to high mortality and larger infarcts compared to all other groups (p < 0.05 to p < 0.01). Pre-treatment by G-CSF (deco) reduced infarct site compared to delayed rt-PA treatment (p < 0.05). G-CSF did not significantly influence PWI when combined with rt-PA. All animals treated by rt-PA showed improved parameters in PWI indicating reperfusion.
Conclusions: G-CSF was neuroprotective when given early after TE. Early combination with rt-PA showed no additional benefit compared to rt-PA or G-CSF alone, but did not lead to side effects. Pretreatment by G-CSF was able to reduce deleterious effects of late rt-PA treatment.
Figures
References
-
- Komine-Kobayashi M, Zhang N, Liu M, Tanaka R, Hara H, Osaka A, Mochizuki H, Mizuno Y, Urabe T. Neuroprotective effect of recombinant human granulocyte colony-stimulating factor in transient focal ischemia of mice. J Cereb Blood Flow Metab. 2006;26:402–13. doi: 10.1038/sj.jcbfm.9600195. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
