

Total and individual coronary artery calcium scores as independent predictors of mortality in hemodialysis patients
- PMID: 20389057
- PMCID: PMC2883846
- DOI: 10.1159/000294405
Total and individual coronary artery calcium scores as independent predictors of mortality in hemodialysis patients
Abstract
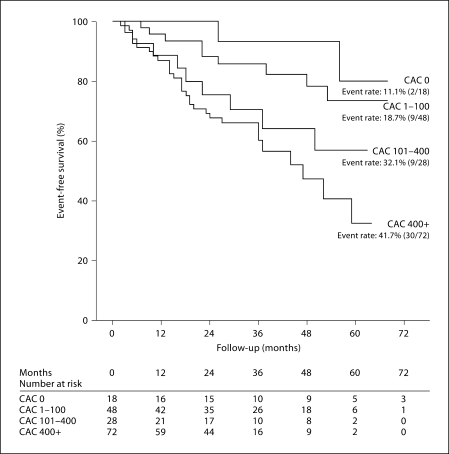
Many traditional and nontraditional risk factors contribute to vascular calcification among maintenance hemodialysis (MHD) patients. It is not clear whether coronary artery calcification (CAC) delineates a higher mortality risk independent of known risk factors. We examined 6-year (10/2001-9/2007) survival of 166 MHD patients, aged 53 +/- 13 years, with baseline CAC scores. Patients were grouped into four CAC groups: 0, 1-100, 101-400, and 400+. The 101-400 and 400+ groups were associated with a significantly higher adjusted risk of death than CAC 0 with hazard ratios (HR) 8.5 (95% CI: 1.1-48.1, p = 0.02) and 13.3 (95% CI: 1.3-65.1, p = 0.01), respectively, independent of demographics, comorbidity, lipids and other cardiovascular risks, surrogates of bone disease, nutritional and inflammatory markers and dialysis dose. Total CAC [HR 6.7 (1.1-21.5, p = 0.03)] followed by the presence of CAC in the left main [4.6 (2.2-9.8, p = 0.001)] and left anterior descending artery [4.3 (2.1-14.2, p = 0.001)] were strong independent predictors of mortality even after adjusting for above covariates. Total and vessel-specific CAC predict mortality in MHD patients independent of traditional and nontraditional risk factors.
2010 S. Karger AG, Basel.
Figures
References
-
- US Renal Data System, USRDS 2008 Annual Data Report . Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2008.
-
- National Kidney Foundation K/DOQI clinical practice guidelines for management of dyslipidemias in patients with kidney. Am J Kidney Dis. 2003;41(suppl 3):S1–S91. - PubMed
-
- Hage FG, Venkataraman R, Zoghbi GJ, Perry GJ, DeMattos AM, Iskandrian AE. The scope of coronary heart disease in patients with chronic kidney disease. J Am Coll Cardiol. 2009;53:2129–2140. - PubMed
-
- Foley RN, Parfrey PS, Sarnak MJ. Epidemiology of cardiovascular disease in chronic renal disease. J Am Soc Nephrol. 1998;9:S16–S23. - PubMed
-
- Zoccali C. Cardiovascular risk in uraemic patients – is it fully explained by classical risk factors? Nephrol Dial Transplant. 2000;15:454–457. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
