

Evaluation of fetuses in a study of intravenous immunoglobulin as preventive therapy for congenital heart block: Results of a multicenter, prospective, open-label clinical trial
- PMID: 20391423
- PMCID: PMC3214993
- DOI: 10.1002/art.27308
Evaluation of fetuses in a study of intravenous immunoglobulin as preventive therapy for congenital heart block: Results of a multicenter, prospective, open-label clinical trial
Abstract
Objective: The recurrence rate of anti-SSA/Ro-associated congenital heart block (CHB) is 17%. Sustained reversal of third-degree block has never been achieved. Based on potential reduction of maternal autoantibody titers as well as fetal inflammatory responses, intravenous immunoglobulin (IVIG) was evaluated as preventive therapy for CHB.
Methods: A multicenter, prospective, open-label study based on Simon's 2-stage optimal design was initiated. Enrollment criteria included the presence of anti-SSA/Ro antibodies in the mother, birth of a previous child with CHB/neonatal lupus rash, current treatment with < or = 20 mg/day of prednisone, and <12 weeks pregnant. IVIG (400 mg/kg) was given every 3 weeks from week 12 to week 24 of gestation. The primary outcome was the development of second-degree or third-degree CHB.
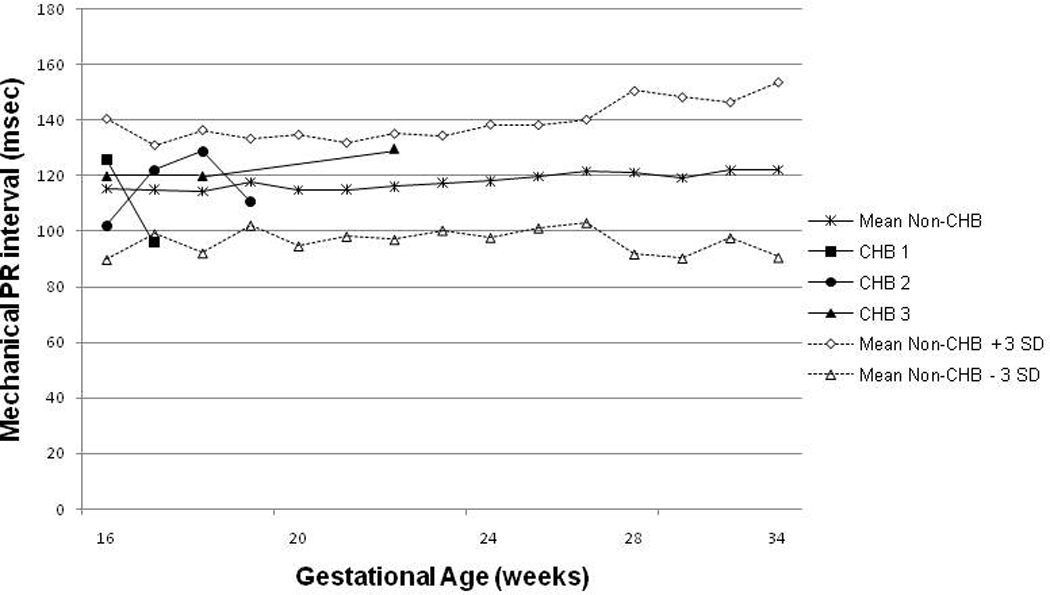
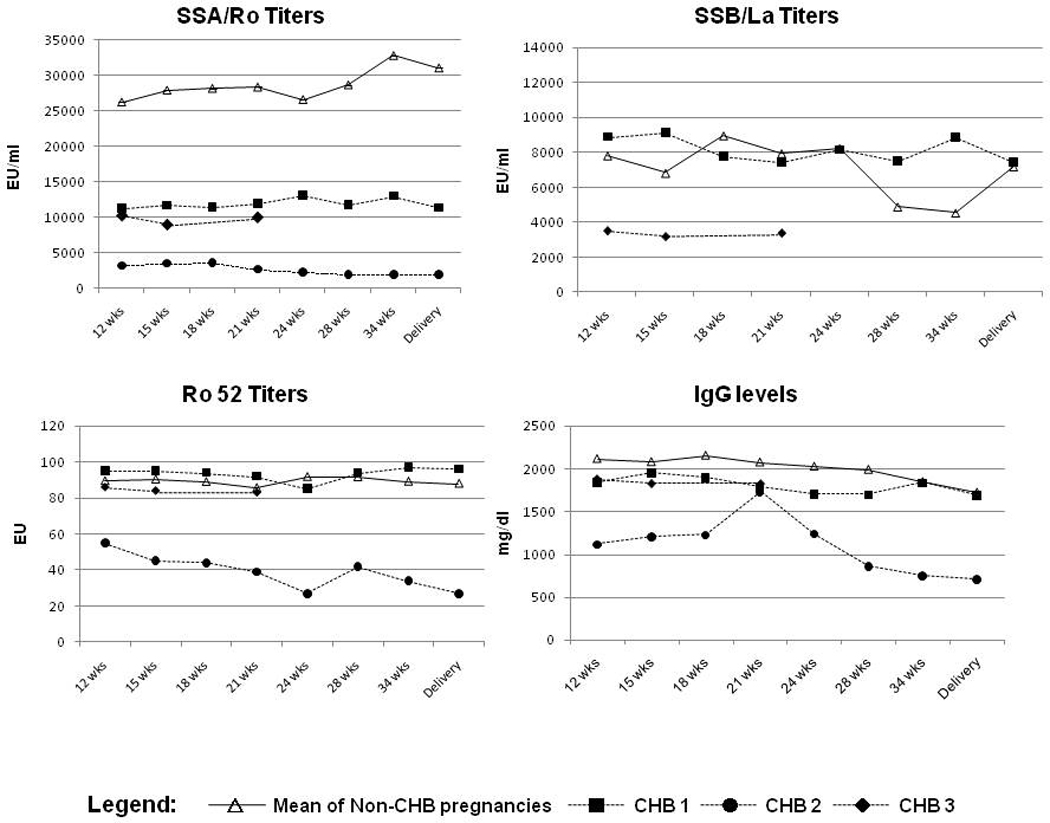
Results: Twenty mothers completed the IVIG protocol before the predetermined stopping rule of 3 cases of advanced CHB in the study was reached. CHB was detected at 19, 20, and 25 weeks; none of the cases occurred following the finding of an abnormal PR interval on fetal Doppler monitoring. One of these mothers had 2 previous children with CHB. One child without CHB developed a transient rash consistent with neonatal lupus. Sixteen children had no manifestations of neonatal lupus at birth. No significant changes in maternal titers of antibody to SSA/Ro, SSB/La, or Ro 52 kd were detected over the course of therapy or at delivery. There were no safety issues.
Conclusion: This study establishes the safety of IVIG and the feasibility of recruiting pregnant women who have previously had a child with CHB. However, IVIG at low doses consistent with replacement does not prevent the recurrence of CHB or reduce maternal antibody titers.
Trial registration: ClinicalTrials.gov NCT00460928.
Figures
References
-
- Brucato A, Frassi M, Franceschini F, Cimaz R, Faden D, Pisoni MP, et al. Risk of Congenital Complete Heart Block in Newborns of Mothers with Anti-Ro/SSA Antibodies Detected by Counterimmunoelectrophoresis. A prospective Study of 100 Women. Arthritis Rheum. 2001;44:1832–1835. - PubMed
-
- Friedman DM, Kim MY, Copel JA, Davis C, Phoon CK, Glickstein JS, et al. Utility of Cardiac Monitoring in Fetuses at Risk for Congenital Heart Block. The PR interval and Dexamethasone evaluation (PRIDE) Prospective Study. Circulation. 2008;117:485–493. - PubMed
-
- Julkunen H, Eronen M. The Rate of Recurrence of Isolated Congenital Heart Block: A Population Based Study. Arthritis Rheum. 2001;44:487–488. - PubMed
-
- Buyon JP, Hiebert R, Copel J, Craft J, Friedman D, Katholi M, et al. Autoimmune-associated congenital heart block: Mortality, morbidity, and recurrence rates obtained from a national neonatal lupus registry. J Am Coll Cardiol. 1998;31:1658–1666. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
