

Impact of the Medicare Modernization Act of 2003 on utilization and spending for medicare part B-covered biologics in rheumatoid arthritis
- PMID: 20391481
- PMCID: PMC3007602
- DOI: 10.1002/acr.20010
Impact of the Medicare Modernization Act of 2003 on utilization and spending for medicare part B-covered biologics in rheumatoid arthritis
Abstract
Objective: To examine changes in utilization and expenditures for infliximab in rheumatoid arthritis (RA) patients associated with the 2 changes implemented by the Medicare Prescription Drug Improvement and Modernization Act (MMA) of 2003, specifically 1) reductions in physician reimbursement for Part B drugs between 2003 and 2005 and 2) availability of alternative RA biologics in 2006.
Methods: Using 2002-2006 5% Medicare files, nationally representative estimates of infliximab use and expenditures were estimated in annual cross-sectional samples of RA beneficiaries. Infliximab initiation and continuation rates were estimated in 2-year longitudinal cohorts (2005-2006 versus 2002-2003, 2003-2004, and 2004-2005).
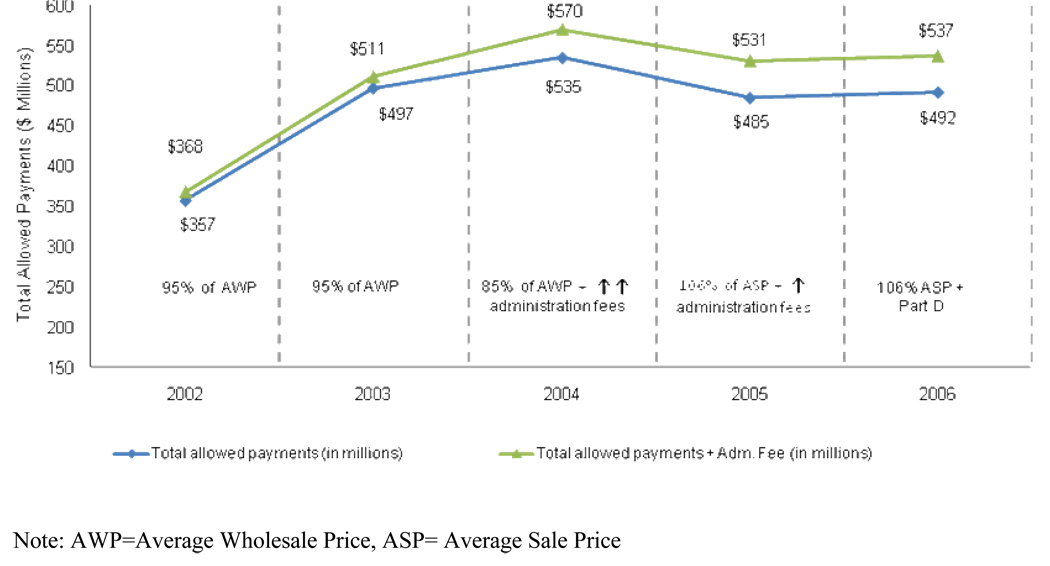
Results: Total payments (in 2006 dollars) for infliximab increased from $357 million in 2002 to $492 million in 2006. The largest annual increase in infliximab payments occurred in the pre-MMA period from 2002 to 2003, wherein payments per RA patient increased by 31%. From 2003 to 2004, despite the reduction in payments brought by the MMA, there was a 4% increase in total expenditures for infliximab per RA patient driven by an increase in utilization factors. Total payments for infliximab per RA patient actually decreased from 2004 to 2005, when reimbursement was further reduced. Continuation and initiation rates for infliximab use remained unchanged in 2006, as compared with previous years.
Conclusion: Infliximab expenditures increased from 2002 to 2006, yet the passage of the MMA was associated with a remarkable slowdown in the rate of increase in expenditures. There was no evidence of significant substitution of infliximab with other biologics made available in 2006.
Figures
Comment in
-
Medicare reimbursement and the use of biologic agents: incentives, access, the public good, and optimal care.Arthritis Care Res (Hoboken). 2010 Mar;62(3):293-5. doi: 10.1002/acr.20088. Arthritis Care Res (Hoboken). 2010. PMID: 20391473 Free PMC article. No abstract available.
References
-
- Office of Inspector General, Department of Health and Human Services. Washington, DC: OIG; 1996. May, Appropriateness of medicare prescription drug allowances. OEI-03-96-00420.
-
- Office of Inspector General, Department of Health and Human Services. Washington, DC: OIG; 1997. May, Appropriateness of medicare prescription drug allowances. OEI-03-96-00420.
-
- Office of Inspector General, Department of Health and Human Services. Washington, DC: OIG; 2001. Jan, Medicare reimbursement of prescription drugs. OEI-03097-00290.
-
- General Accounting Office. Washington, DC: 2001. Sep, Medicare: Payments for covered outpatient drugs exceed providers' cost. GAO-011118.
-
- Danzon PM, Wilensky GR, Means KE. Alternative strategies for medicare payment of outpatient prescription drugs--part B and beyond. Am J Manag Care. 2005;11(3):173–180. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
