

Aspirin with or without an antiemetic for acute migraine headaches in adults
- PMID: 20393963
- PMCID: PMC4163048
- DOI: 10.1002/14651858.CD008041.pub2
Aspirin with or without an antiemetic for acute migraine headaches in adults
Update in
-
Aspirin with or without an antiemetic for acute migraine headaches in adults.Cochrane Database Syst Rev. 2013 Apr 30;2013(4):CD008041. doi: 10.1002/14651858.CD008041.pub3. Cochrane Database Syst Rev. 2013. PMID: 23633350 Free PMC article.
Abstract
Background: Migraine is a common, disabling condition and a burden for the individual, health services and society. Many sufferers choose not to, or are unable to, seek professional help and rely on over-the-counter analgesics. Co-therapy with an antiemetic should help to reduce nausea and vomiting commonly associated with migraine headaches.
Objectives: To determine the efficacy and tolerability of aspirin, alone or in combination with an antiemetic, compared to placebo and other active interventions in the treatment of acute migraine headaches in adults.
Search strategy: We searched Cochrane CENTRAL, MEDLINE, EMBASE and the Oxford Pain Relief Database for studies through 10 March 2010.
Selection criteria: We included randomised, double-blind, placebo- or active-controlled studies using aspirin to treat a discrete migraine headache episode, with at least 10 participants per treatment arm.
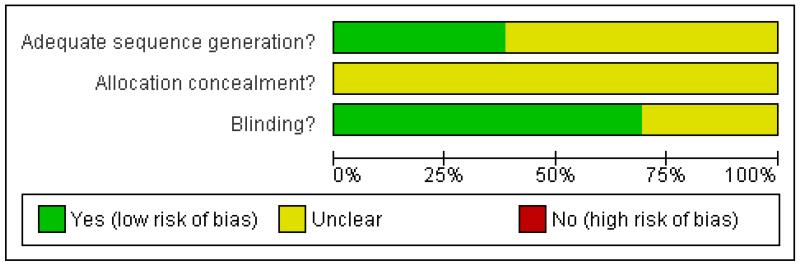
Data collection and analysis: Two review authors independently assessed trial quality and extracted data. Numbers of participants achieving each outcome were used to calculate relative risk and numbers needed to treat (NNT) or harm (NNH) compared to placebo or other active treatment.
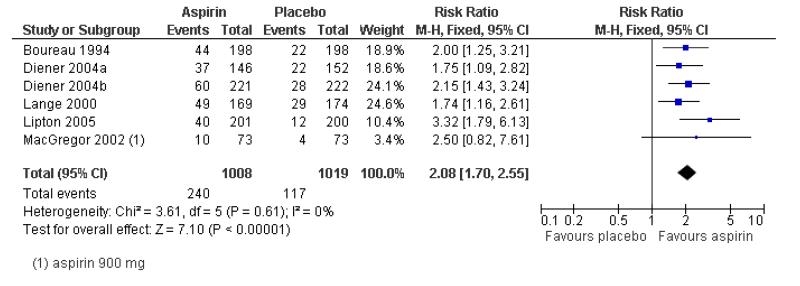
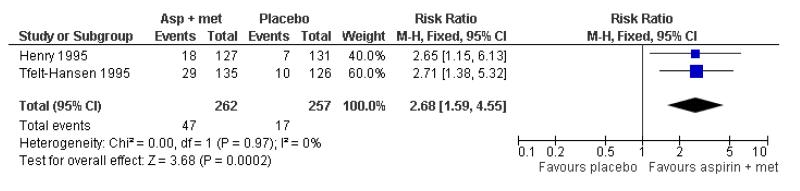
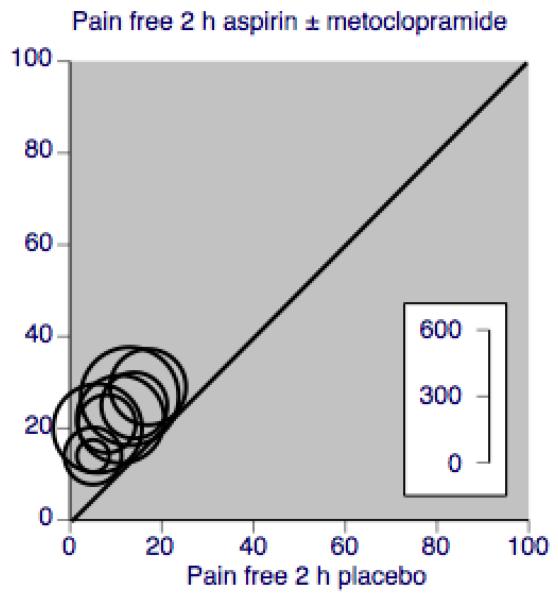
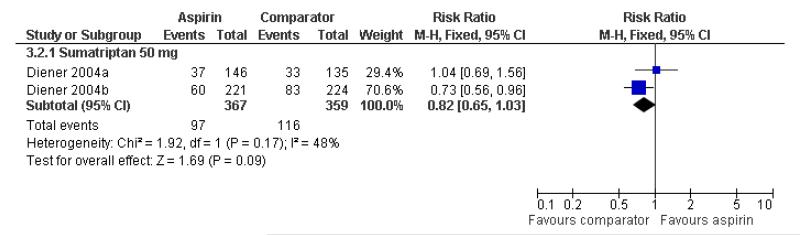
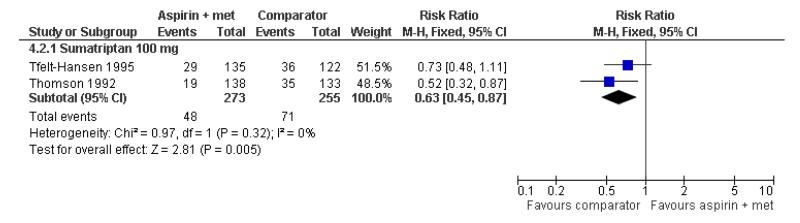
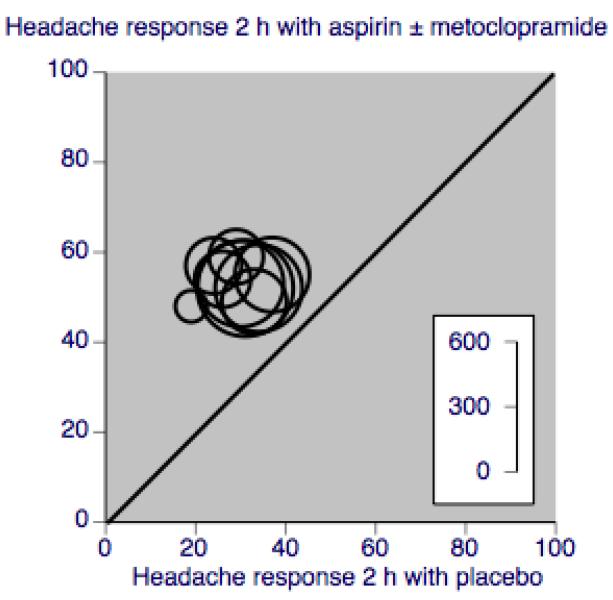
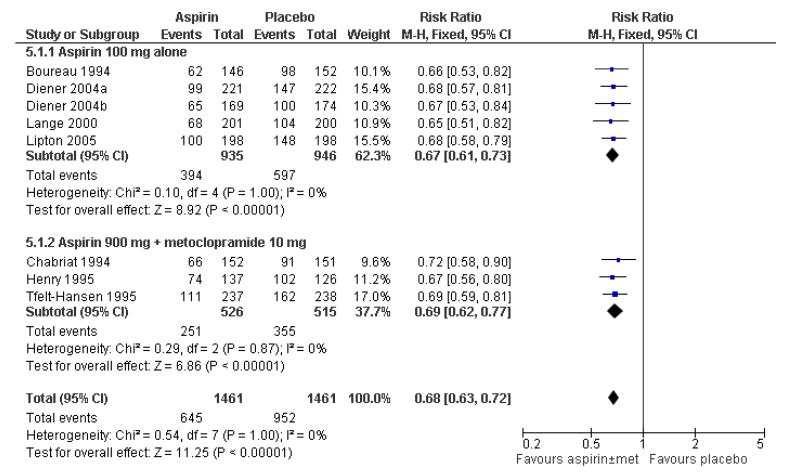
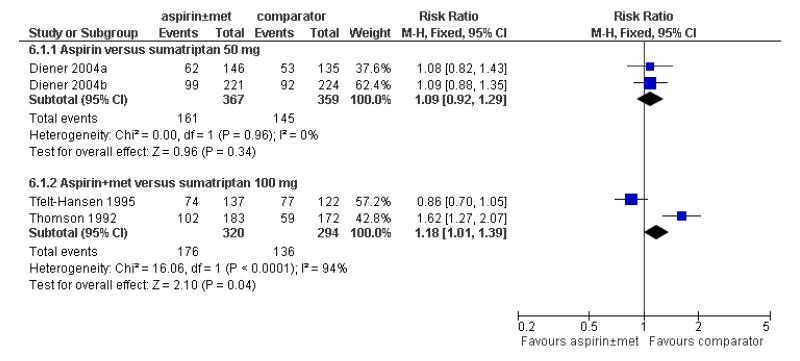
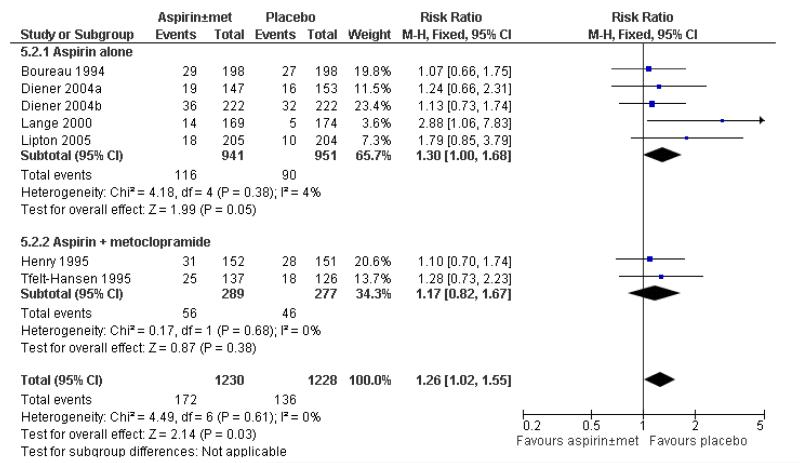
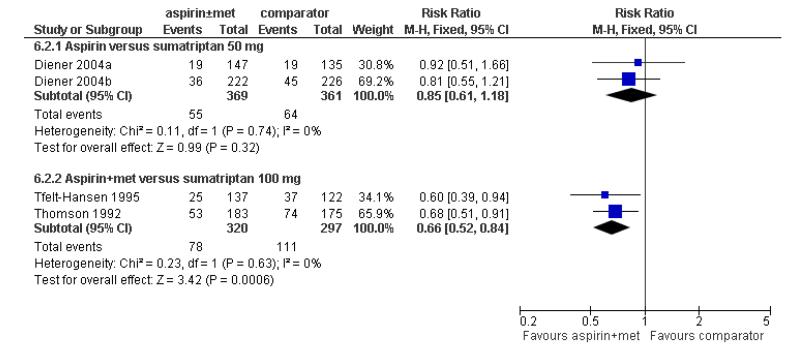
Main results: Thirteen studies (4222 participants) compared aspirin 900 mg or 1000 mg, alone or in combination with metoclopramide 10 mg, with placebo or other active comparators, mainly sumatriptan 50 mg or 100 mg. For all efficacy outcomes, all active treatments were superior to placebo, with NNTs of 8.1, 4.9 and 6.6 for 2-hour pain-free, 2-hour headache relief, and 24-hour headache relief with aspirin alone versus placebo, and 8.8, 3.3 and 6.2 with aspirin plus metoclopramide versus placebo. Sumatriptan 50 mg did not differ from aspirin alone for 2-hour pain-free and headache relief, while sumatriptan 100 mg was better than the combination of aspirin plus metoclopramide for 2-hour pain-free, but not headache relief; there were no data for 24-hour headache relief.Associated symptoms of nausea, vomiting, photophobia and phonophobia were reduced with aspirin compared with placebo, with additional metoclopramide significantly reducing nausea (P < 0.00006) and vomiting (P = 0.002) compared with aspirin alone.Fewer participants needed rescue medication with aspirin than with placebo. Adverse events were mostly mild and transient, occurring slightly more often with aspirin than placebo.
Authors' conclusions: Aspirin 1000 mg is an effective treatment for acute migraine headaches, similar to sumatriptan 50 mg or 100 mg. Addition of metoclopramide 10 mg improves relief of nausea and vomiting. Adverse events were mainly mild and transient, and were slightly more common with aspirin than placebo, but less common than with sumatriptan 100 mg.
Figures
Comment in
-
ACP Journal Club. Review: Aspirin reduces acute migraine pain in adults.Ann Intern Med. 2010 Nov 16;153(10):JC5-5. doi: 10.7326/0003-4819-153-10-201011160-02005. Ann Intern Med. 2010. PMID: 21079212 No abstract available.
-
Aspirin with or without an anti-emetic for migraine headaches in adults.Int J Evid Based Healthc. 2011 Mar;9(1):74-5. doi: 10.1111/j.1744-1609.2010.00206.x. Int J Evid Based Healthc. 2011. PMID: 21332668 No abstract available.
References
References to studies included in this review
-
- Boureau F, Joubert JM, Lasserre V, Prum B, Delecoeuillerie G. Double-blind comparison of an acetaminophen 400 mg-codeine 25 mg combination versus aspirin 1000 mg and placebo in acute migraine attack. Cephalalgia. 1994;14(2):156–61. - PubMed
-
- Chabriat H, Joire JE, Danchot J, Grippon P, Bousser MG. Combined oral lysine acetylsalicylate and metoclopramide in the acute treatment of migraine: a multicentre double-blind placebo-controlled study. Cephalalgia. 1994;14(4):297–300. - PubMed
-
- Diener HC, Eikermann A, Gessner U, Göbel H, Haag G, Lange R, et al. Efficacy of 1,000 mg effervescent acetylsalicylic acid and sumatriptan in treating associated migraine symptoms. European Neurology. 2004;52(1):50–6. [DOI: 10.1159/000079544] - PubMed
-
- Diener HC, Bussone G, de Liano H, Eikermann A, Englert R, Floeter T, et al. EMSASI Study Group. Placebo-controlled comparison of effervescent acetylsalicylic acid, sumatriptan and ibuprofen in the treatment of migraine attacks. Cephalalgia. 2004;24(11):947–54. [DOI: 10.1111/j.1468-2982.2004.00783.x] - PubMed
-
- Geraud G, Compagnon A, Rossi A, COZAM Study Group Zolmitriptan versus a combination of acetylsalicylic acid and metoclopramide in the acute oral treatment of migraine: a double-blind, randomised, three-attack study. European Neurology. 2002;47(2):88–98. - PubMed
References to studies excluded from this review
-
- Chabriat H, Joire JE, Danchot J, Bousser MG. Association of aspirin and metoclopramide in the treatment of migraine attacks. Cephalagia. 1993;13(13):96.
-
- Diener HC, Pfaffenrath V, Pageler L, Peil H, Aicher B. The fixed combination of acetylsalicylic acid, paracetamol and caffeine is more effective than single substances and dual combination for the treatment of headache: a multicentre, randomized, double-blind, single-dose, placebo-controlled parallel group study. Cephalalgia. 2005;25(10):776–87. - PubMed
-
- Limmroth V, May A, Diener H. Lysine-acetylsalicylic acid in acute migraine attacks. European Neurology. 1999;41(2):88–93. - PubMed
-
- Nebe J, Heier M, Diener HC. Low-dose ibuprofen in self-medication of mild to moderate headache: a comparison with acetylsalicylic acid and placebo. Cephalalgia. 1995;15(6):531–5. - PubMed
-
- Tfelt-Hansen P, Olesen J. Paracetamol (acetaminophen) versus acetylsalicylic acid in migraine. European Neurology. 1980;19(3):163–5. - PubMed
Additional references
-
- Bigal ME, Serrano D, Reed M, Lipton RB. Chronic migraine in the population: burden, diagnosis, and satisfaction with treatment. Neurology. 2008;71(8):559–66. [DOI: 10.1212/01.wnl.0000323925.29520.e7] - PubMed
-
- Clarke CE, MacMillan L, Sondhi S, Wells NEJ. Economic and social impact of migraine. The Quarterly Journal of Medicine. 1996;89(1):77–84. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical