

Survival after application of automatic external defibrillators before arrival of the emergency medical system: evaluation in the resuscitation outcomes consortium population of 21 million
- PMID: 20394876
- PMCID: PMC3008654
- DOI: 10.1016/j.jacc.2009.11.077
Survival after application of automatic external defibrillators before arrival of the emergency medical system: evaluation in the resuscitation outcomes consortium population of 21 million
Abstract
Objectives: The purpose of this study was to assess the effectiveness of contemporary automatic external defibrillator (AED) use.
Background: In the PAD (Public Access Defibrillation) trial, survival was doubled by focused training of lay volunteers to use an AED in high-risk public settings.
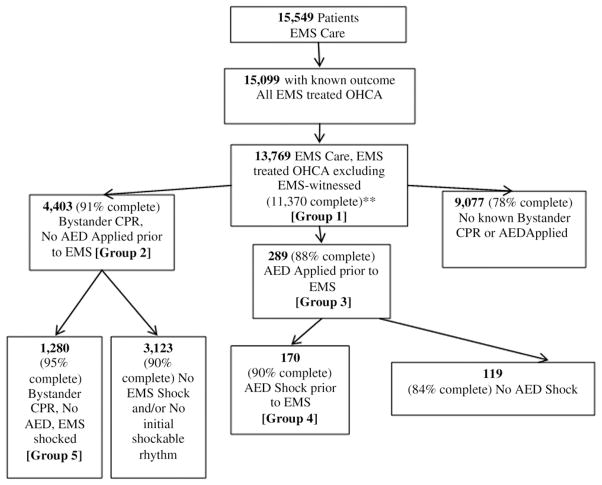
Methods: We performed a population-based cohort study of persons with nontraumatic out-of-hospital cardiac arrest before emergency medical system (EMS) arrival at Resuscitation Outcomes Consortium (ROC) sites between December 2005 and May 2007. Multiple logistic regression was used to assess the independent association between AED application and survival to hospital discharge.
Results: Of 13,769 out-of-hospital cardiac arrests, 4,403 (32.0%) received bystander cardiopulmonary resuscitation but had no AED applied before EMS arrival, and 289 (2.1%) had an AED applied before EMS arrival. The AED was applied by health care workers (32%), lay volunteers (35%), police (26%), or unknown (7%). Overall survival to hospital discharge was 7%. Survival was 9% (382 of 4,403) with bystander cardiopulmonary resuscitation but no AED, 24% (69 of 289) with AED application, and 38% (64 of 170) with AED shock delivered. In multivariable analyses adjusting for: 1) age and sex; 2) bystander cardiopulmonary resuscitation performed; 3) location of arrest (public or private); 4) EMS response interval; 5) arrest witnessed; 6) initial shockable or not shockable rhythm; and 7) study site, AED application was associated with greater likelihood of survival (odds ratio: 1.75; 95% confidence interval: 1.23 to 2.50; p < 0.002). Extrapolating this greater survival from the ROC EMS population base (21 million) to the population of the U.S. and Canada (330 million), AED application by bystanders seems to save 474 lives/year.
Conclusions: Application of an AED in communities is associated with nearly a doubling of survival after out-of-hospital cardiac arrest. These results reinforce the importance of strategically expanding community-based AED programs.
Copyright (c) 2010 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Shah JS, Maisel WH. Recalls and safety alerts affecting automated external defibrillators. JAMA. 2006;296:655–60. - PubMed
-
- Valenzuela TD, Roe DJ, Nichol G, Clark LL, Spaite DW, Hardman RG. Outcomes of rapid defibrillation by security officers after cardiac arrest in casinos. N Engl J Med. 2000;343:1206–9. - PubMed
-
- Page RL, Joglar JA, Kowal RC, et al. Use of automated external defibrillators by a U.S. airline. N Engl J Med. 2000;343:1210–6. - PubMed
-
- White RD, Hankins DG, Bugliosi TF. Seven years’ experience with early defibrillation by police and paramedics in an emergency medical services system. Resuscitation. 1998;39:145–51. - PubMed
-
- Caffrey SL, Willoughby PJ, Pepe PE, Becker LB. Public use of automated external defibrillators. N Engl J Med. 2002;347:1242–7. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HL077866/HL/NHLBI NIH HHS/United States
- HL077867/HL/NHLBI NIH HHS/United States
- 5U01 HL077863/HL/NHLBI NIH HHS/United States
- HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- HL077873/HL/NHLBI NIH HHS/United States
- HL077871/HL/NHLBI NIH HHS/United States
- HL077881/HL/NHLBI NIH HHS/United States
- HL077908/HL/NHLBI NIH HHS/United States
- U01 HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- CAPMC/ CIHR/Canada
- U01 HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
- HL077872/HL/NHLBI NIH HHS/United States
- HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- HL077885/HL/NHLBI NIH HHS/United States
- HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
