

Increased whole-body adiposity without a concomitant increase in liver fat is not associated with augmented metabolic dysfunction
- PMID: 20395947
- PMCID: PMC3319734
- DOI: 10.1038/oby.2010.90
Increased whole-body adiposity without a concomitant increase in liver fat is not associated with augmented metabolic dysfunction
Abstract
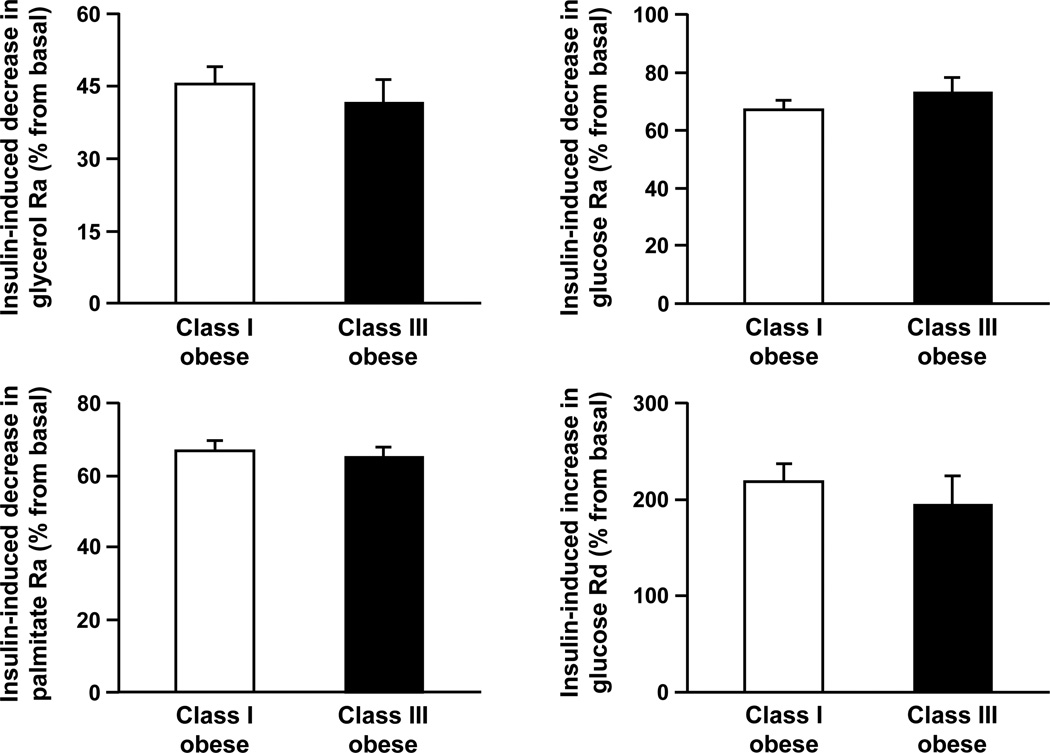
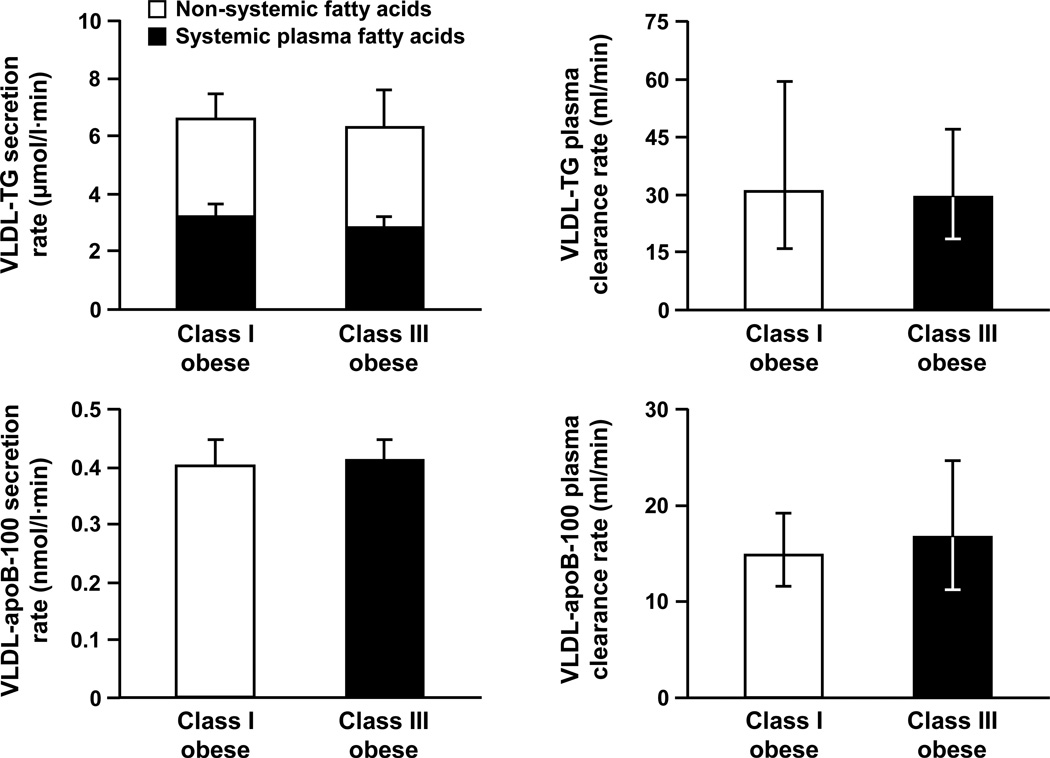
Aim of this study was to determine whether an increase in adiposity, without a concomitant increase in intrahepatic triglyceride (IHTG) content, is associated with a deterioration in metabolic function. To this end, multiorgan insulin sensitivity, assessed by using a two-stage hyperinsulinemic-euglycemic clamp procedure in conjunction with stable isotopically labeled tracer infusion, and very low-density lipoprotein (VLDL) kinetics, assessed by using stable isotopically labeled tracer infusion and mathematical modeling, were determined in 10 subjects with class I obesity (BMI: 31.6 +/- 0.3 kg/m(2); 37 +/- 2% body fat; visceral adipose tissue (VAT): 1,225 +/- 144 cm(3)) and 10 subjects with class III obesity (BMI: 41.5 +/- 0.5 kg/m(2); 43 +/- 2% body fat; VAT: 2,121 +/- 378 cm(3)), matched on age, sex, and IHTG content (14 +/- 4 and 14 +/- 3%, respectively). No differences between class I and class III obese groups were detected in insulin-mediated suppression of palmitate (67 +/- 3 and 65 +/- 3%, respectively; P = 0.635) and glucose (67 +/- 3 and 73 +/- 5%, respectively; P = 0.348) rates of appearance in plasma, and the insulin-mediated increase in glucose disposal (218 +/- 18 and 193 +/- 30%, respectively; P = 0.489). In addition, no differences between class I and class III obese groups were detected in secretion rates of VLDL-triglyceride (6.5 +/- 1.0 and 6.0 +/- 1.4 micromol/l x min, respectively; P = 0.787) and VLDL-apolipoprotein B-100 (0.40 +/- 0.05 and 0.41 +/- 0.04 nmol/l x min, respectively; P = 0.866), and plasma clearance rates of VLDL-triglyceride (31 (16-59) and 29 (18-46) ml/min, respectively; P = 0.888) and VLDL-apolipoprotein B-100 (15 (11-19) and 17 (11-25) ml/min, respectively; P = 0.608). We conclude that increased adiposity without a concomitant increase in IHTG content does not cause additional abnormalities in adipose tissue, skeletal muscle, and hepatic insulin sensitivity, or VLDL metabolism.
Conflict of interest statement
Disclosure: There are no financial conflicts with the subject matter or materials discussed in this manuscript with any of the authors.
Figures
References
-
- Klein S, Wadden T, Sugerman HJ. AGA technical review on obesity. Gastroenterology. 2002;123:882–932. - PubMed
-
- National Institutes of Health. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults - The Evidence Report. Obes Res. 1998;6 Suppl 2:51S–209S. - PubMed
-
- Gallagher D, Heymsfield SB, Heo M, Jebb SA, Murgatroyd PR, Sakamoto Y. Healthy percentage body fat ranges: an approach for developing guidelines based on body mass index. Am J Clin Nutr. 2000;72:694–701. - PubMed
-
- Gallagher D, Visser M, Sepulveda D, Pierson RN, Harris T, Heymsfield SB. How useful is body mass index for comparison of body fatness across, age, sex, and ethnic groups? Am J Epidemiol. 1996;143:228–239. - PubMed
-
- Colditz GA, Willett WC, Stampfer MJ, Manson JE, Hennekens CH, Arky RA, et al. Weight as a risk factor for clinical diabetes in women. Am J Epidemiol. 1990;132:501–513. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
