

Chemotherapy with laparoscope-assisted continuous circulatory hyperthermic intraperitoneal perfusion for malignant ascites
- PMID: 20397270
- PMCID: PMC2856833
- DOI: 10.3748/wjg.v16.i15.1901
Chemotherapy with laparoscope-assisted continuous circulatory hyperthermic intraperitoneal perfusion for malignant ascites
Abstract
Aim: To investigate the procedure, feasibility and effects of laparoscope-assisted continuous circulatory hyperthermic intraperitoneal perfusion chemotherapy (CHIPC) in treatment of malignant ascites induced by peritoneal carcinomatosis from gastric cancers.
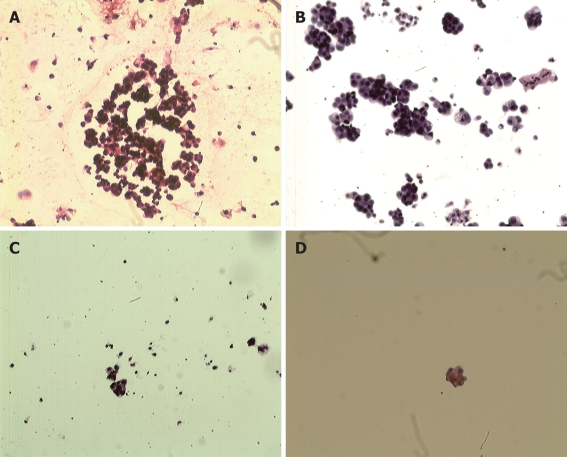
Methods: From August 2006 to March 2008, the laparoscopic approach was used to perform CHIPC on 16 patients with malignant ascites induced by gastric cancer or postoperative intraperitoneal seeding. Each patient underwent CHIPC three times after laparoscope-assisted perfusion catheters placing. The first session was completed in operative room under general anesthesia, 5% glucose solution was selected as perfusion liquid, and 1500 mg 5-fluorouracil (5-FU) and 200 mg oxaliplatin were added in the perfusion solution. The second and third sessions were performed in intensive care unit, 0.9% sodium chloride solution was selected as perfusion liquid, and 1500 mg 5-FU was added in the perfusion solution alone. CHIPC was performed for 90 min at a velocity of 450-600 mL/min and an inflow temperature of 43 +/- 0.2 degrees C.
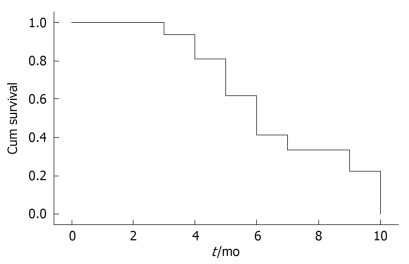
Results: The intraoperative course was uneventful in all cases, and the mean operative period for laparoscope-assisted perfusion catheters placing was 80 min for each case. No postoperative deaths or complications related to laparoscope-assisted CHIPC occurred in this study. Clinically complete remission of ascites and related symptoms were achieved in 14 patients, and partial remission was achieved in 2 patients. During the follow-up, 13 patients died 2-9 mo after CHIPC, with a median survival time of 5 mo. Two patients with partial remission suffered from port site seeding and tumor metastasis,and died 2 and 3 mo after treatment. Three patients who are still alive today survived 4, 6 and 7 mo, respectively. The Karnofsky marks of patients (50-90) increased significantly (P < 0.01) and the general status improved after CHIPC. Thus satisfactory clinical efficacy has been achieved in these patients treated by laparoscopic CHIPC.
Conclusion: Laparoscope-assisted CHIPC is a safe, feasible and effective procedure in the treatment of debilitating malignant ascites induced by unresectable gastric cancers.
Keywords: Chemotherapy; Gastric cancer; Intraperitoneal hyperthermic perfusion; Laparoscopy; Malignant ascites.
Figures
References
-
- Patriti A, Cavazzoni E, Graziosi L, Pisciaroli A, Luzi D, Gullà N, Donini A. Successful palliation of malignant ascites from peritoneal mesothelioma by laparoscopic intraperitoneal hyperthermic chemotherapy. Surg Laparosc Endosc Percutan Tech. 2008;18:426–428. - PubMed
-
- Kusamura S, Younan R, Baratti D, Costanzo P, Favaro M, Gavazzi C, Deraco M. Cytoreductive surgery followed by intraperitoneal hyperthermic perfusion: analysis of morbidity and mortality in 209 peritoneal surface malignancies treated with closed abdomen technique. Cancer. 2006;106:1144–1153. - PubMed
-
- Deraco M, Casali P, Inglese MG, Baratti D, Pennacchioli E, Bertulli R, Kusamura S. Peritoneal mesothelioma treated by induction chemotherapy, cytoreductive surgery, and intraperitoneal hyperthermic perfusion. J Surg Oncol. 2003;83:147–153. - PubMed
-
- Levine EA, Stewart JH 4th, Russell GB, Geisinger KR, Loggie BL, Shen P. Cytoreductive surgery and intraperitoneal hyperthermic chemotherapy for peritoneal surface malignancy: experience with 501 procedures. J Am Coll Surg. 2007;204:943–953; discussion 953-955. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
